Mark Klimek Lectures 1 To 12 Nursing Notes

GUIDE • Mark Klimek’s Lecture
| Lecture 1— | Acid-Base Balance | Dumping/HH | |
| Ventilators | Electrolytes: K+, CA, MG, | ||
| and NA | |||
| Lecture 2— | Alcohol | TX for HyperKalemia | |
| Wernicke | |||
| Overdose and Withdrawal | Lecture 7— | Thyroid (Hyper-, Hypo-) | |
| S/Sx | Adrenal Cortex (Addison | ||
| Aminoglycosides | Disease, Cushing) | ||
| Peak and Trough | Toys | ||
| Laminectomy | |||
| Lecture 3— | Drug Toxicities (Lithium, | ||
| Lanoxin, Dilantin, Bilirubin, | Lecture 8— | Lab Values | |
| Aminophylline) | Five Deadly Ds | ||
| Kernicterus | Neutropenic Precaution | ||
| Dumping/HH | |||
| Electrolytes: K+, CA, MG, | Lecture 9— | Psych Drugs | |
| and NA | Tri | ||
| TX for HyperKalemia | Benzo | ||
| MAOI | |||
| Lecture 4— | Crutches | Lithium | |
| Canes | Prozac | ||
| Walkers | Haldol | ||
| Delusions | Clozaril | ||
| Hallucinations | Zoloft | ||
| Psychosis | |||
| Psychotic and Non-Psychotic | Lecture 10— | Maternity and Neonatology | |
| Hallucination | |||
| Illusion | Lecture 11— | Fetal Complications | |
| Delusion | Stages of Labor | ||
| Assessments | |||
| Lecture 5— | Diabetes Mellitus | Variations for NB | |
| Diabetes Insipidus | Maternity Meds | ||
| SIADH | Medication Hints | ||
| Insulin | Psych Tips | ||
| DKA | Operational Stages | ||
| HHNK | |||
| Lecture 12— | Prioritization | ||
| Lecture 6— | Drug Toxicities (Lithium, | Delegation | |
| Lanoxin, Dilantin, Bilirubin, | Staff Management | ||
| Aminophylline) | Guessing Strategies | ||
| Kernicterus |
Lecture 1 • Mark Klimek • 92:21
Acid/Base Balance (Start times: 30:00)
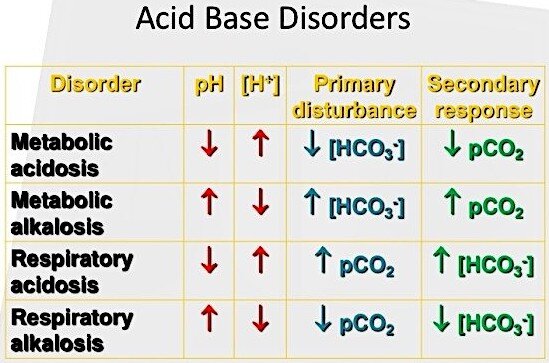
In order to solve acid-base disorders, it is important to know the normal values for pH, CO2 and HCO3 (bicarbonate), which are shown below
- pH 7.35 to 7.45
- CO2 35 to 45
- HCO3 22 to 26
The first value to look at in an acid-base disorder is the pH
- If pH is <7.35, the acid-base imbalance is acidotic
- If pH is <7.45, the acid-base imbalance is alkalotic
Now, to determine if the imbalance is metabolic or respiratory, determine whether HCO3 goes in the same or opposite direction with pH
- Rule of the Bs: If pH and Bicarb move both in the same direction, then the acid-base imbalance is metabolic … Otherwise, it is respiratory
Example #1
- pH 7.3 Acidotic
- HCO3 20 Metabolic
- This is an example of metabolic acidosis
Example #2
- pH 7.58 Alkalotic
- HCO3 32 Metabolic
- This is an example of metabolic alkalosis
Example #3
- pH 7.22 Acidosis
- HCO3 35 Respiratory
- This is an example of respiratory acidosis
As the pH goes, so goes my patient, except for Potassium … That means
- If pH is low, everything is low, except potassium
- If pH is high, everything is high, except potassium
If pH goes over 7.45, this is alkalosis
- Therefore everything is up: tachycardia, tachypnea, HTN, seizures, irritability, spastic, diarrhea, borborygmi (increase bowel sounds), hyperreflexia (3+, 4+)
- However, potassium is opposite. Therefore, hypokalemia
- What is the nursing intervention?
- Pt need suctioning because of seizures
If pH goes below 7.35, this is acidosis
- Therefore, everything is down: bradycardia, constipation, absent bowel sounds, flaccid, obtunded, lethargy, coma hyporeflexia (0, 1+), bradypnea, low BP
- However, potassium is high (hyperkalemia)
- What is the nursing intervention?
- Pt needs to be ventilated with an Ambu bag—respiratory arrest
So, remember that “MAC Kussmaul” is the only acid-base imbalance to cause Metabolic ACidosis with Kussmaul respirations
Causes of Acid/Base imbalance
First ask yourself, “Is it LUNG? … If yes, then it is respiratory
- Then ask yourself, “Are they overventilating or underventilating?
- If UNDERventilating, then pick acidosis—pH is under 7.35
- If OVERventilating, then it is alkalosis, pH is over 7.45
What type of acid-base derangement is present in the following condition?
- In labor?
- Respiratory alkalosis … Overventilating—pH increases … Alkalosis)
- Drowning?
- Respiratory acidosis … Underventilating—pH decreases … Acidosis
- Pt is on PCA (patient-controlled anesthesia) pump?

- Ventilation is down … Respiratory acidosis
If it is not LUNG, then it is metabolic. If the patient has prolonged gastric vomiting or suction (sucking out acid), pick alkalosis
- For everything else that isn’t lung, pick metabolic acidosis
So, when you don’t know what to pick, pick metabolic acidosis
Tip
- Set your default setting to Metabolic Acidosis
- Always pay attention to modifying phrase rather than original noun
Figure 1. Patient- controlled anesthesia (PCA) pump.
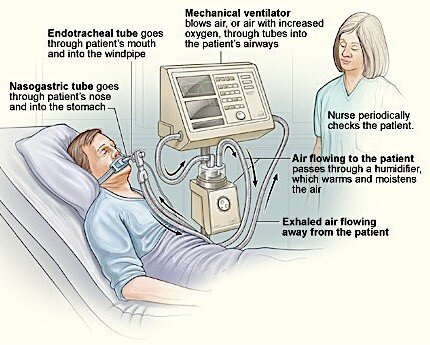
Ventilator
A ventilator is a machine designed to move breathable air into and out of the lungs, aids patients who are physically unable to breathe, or breathing insufficiently to breathe … A ventilators is equipped with a high and a low-pressure alarm
High pressures alarms are always triggered by increased resistance to air flow. Look for obstructions, i.e.,
- Kinks in tubing … Solution: unkink the tube
- Condensed water in the dependent tube … Solution: empty it
- Mucus plugs … Solution: Ask pt to turn, cough, deep breathe; or suction the tubing PRN
What is the appropriate order to address high pressure alarm in a mechanical ventilator?
- (1) Unkink. (2) Empty water out of tubing. (3) turn pt, ask pt to cough or deeply breathe, and (4) suction
Low pressures alarms are always triggered by decrease in resistance. This can be caused by
- Main tubing disconnection
- O2 sensor tube disconnection
- In both cases, reconnect the disconnected tubing unless tube is on floor … Bag pt and call Respiratory Therapist
The ventilator may be set too high or too low
- Setting is too high … Pt is overventilated
- Respiratory Alkalosis … Panting
- Setting is too low … Pt is underventilated
- Respiratory Acidosis … Pt is retaining CO2
Question
The physician wants to wean pt off vent in the morning. At 6 am, the ABGs say respiratory acidosis. What would you do next?
- Notify the physician that the pt is not ready to be weaned off the respirator
- Pt is is respiratory acidosis, which means that he is underventilated … Therefore not ready to be weaned off the ventilator
- If pt were in respiratory alkalosis (overventilated), he should be ready to be weaned off
Lecture 2 • Mark Klimek • 101:54
Alcoholism
- The #1 psychological problem is DENIAL
The title of this section is alcoholism. However, this rule can be used for any abuse situation
- So, what it the number 1 psychological problem in child abuse? … In gambling?
… In cocaine abuse? … In spousal abuse? … In elder abuse?
a. The answer is denial
- How do you respond/treat to pts in denial?
- Confront them by pointing out the difference b/w what they say and what they do
- For instance, say something like: “Ok, you say you’re not an alcoholic but it is 10 a.m. and you’ve already had a 6 pack” … It is not the same as aggression. Don’t attack the person
- Good answer has “I” … Bad answer has “YOU”
- One place where denial is ok—loss and grief Stages of grief are “DABDA”—Denial, anger, bargaining, depression, acceptance
- So when the question is about pt in denial, pay attention to whether you are dealing with
loss or abusive situation Support = Loss Confront = Abuse
Dependency vs. Co-dependency
- The #2 psychological problem is Dependency or Co-Dependency
- Dependency: when the get the significant other to do things or make decisions for them
- The abuser is dependent
- Co-dependency: when the significant other derive self-esteem for doing things or making decisions for the abuser
- The significant other is the co-dependent
Dependency and co-dependency has a symbiotic, yet a pathological relationship
-
- The dependent pt get a free ride on the co-dependent
- The co-defendant pt feels good from “doing stuff” for the abuser
- How do you treat dependency/codependency?
- Dependent pts are “abusers” … Confront them
- Co-dependent pts have self-esteem issues … Teach pts how to set limits and enforce them
- Agree in advance on what requests are allowed then enforce
- Teach significant other to say no
- Work on self-esteem on the co-dependent person
Manipulation
- Manipulation is when the abuser gets the significant other to do things or make decisions that are not in the best interests of the significant other
- The nature of the act is dangerous and harmful to the significant other
- How is manipulation like dependency?
- In both situations the dependent person gets the co-dependent person to do things or make decisions
- If what the significant other is being asked to do is not inherently dangerous and harmful, then this is dependency/co-dependency
- However, if the significant other is being asked to do something inherently dangerous and harmful, then this is manipulation
- Manipulation? Set LIMITS and Enforce them
Examples
Determine if either one of these situations is dependent/co-dependent problem or a manipulation problem
- A 49-year-old alcoholic gets her 17-year-old son to go to the store and buy alcohol for her.
- The mother is manipulating the son
- This is an illegal act = Harmful
- Dependency … There are 2 patients
- The dependent has a denial issue
- The co-dependent has a self-esteem issue
- A 49-year-old alcoholic asks her 50-year-old husband to go to the store and buy alcohol for her.
- This is not illegal for the husband to buy alcohol
- This a dependency/co-dependency situation
- Manipulation … There is 1 patient—no self-esteem issues
- Easier to treat because no one like to be manipulated
Wernicke (Korsakoff) Syndrome
Typically, Wernicke and Korsafoff are 2 separate disorders. The NCLEX however bundles the 2 as 1 condition
- Wernicke is an encephalopathy
- Korsakoff is a psychosis
- Wernicke and Korsafoff tend to go together
Wernicke and Korsafoff
- Psychosis induced by Vitamin B1, thiamine deficiency
- This is a situation the pt looses touch with reality due to vit B1 deficiency
- The primary S/Sx are amnesia (memory loss) and confabulation (making up stories)
- Confabulation—The lies for this pts are just as real as reality
How do deal with a pt with Wernicke and Korsafoff who is confabulating about going to a meeting with Barack Obama this morning?
- Redirect the pt to something he can do
- For instance, tell pt something along that line: “Why can we go watch TV to see what is on the news today”
Characteristics of Wernicke and Korsafoff syndrome
- Preventable … Take B1
- Arrestable (stop it from getting worse) … Take B1
- Irreversible (70%) … Will kill brain cells
Antabuse and Revia (Disulfiram)
- Antabuse—Alcohol deterrent
- Revia—Antidote
- Aversion (strong hatred) Therapy—a type of behavior therapy designed to make a patient give up an undesirable habit by causing them to associate it with an unpleasant effect
- Works in theory better than in reality
- Onset (how long it takes to start working) and duration (how long it lasts) of effectiveness of Antabuse/Revia is 2 weeks
- For instance, if pt will be at a function and would like to drink, the pt must be on Antabuse/Revia at least 2 weeks prior to the event
- Patient teaching
- Teach pt to avoid all forms of EtOH. Not doing so may lead to symptoms of n/v, even death
- Teach them to avoid the followings items as they contain alcohol … Mouth wash, cologne, perfume, aftershave, elixir, most OTC liquid medicine, insect repellant, hand sanitizer, vanilla extract (can’t have cupcake with unbaked icing)
On the exam, do not pick the Red Wine vinaigrettes … It does not have alcohol in it
Overdose and Withdrawal
First thing you ask in an overdose question is: Is it an Upper or a Downer?
- This is because every abuse drug is either an Upper or a Downer
- However, laxative abuse in the elderly is neither an Upper nor a Downer
Upper Downer
- Caffeine
- Cocaine
- PCP/LSD (psychedelics/hallucinogens)
- Methamphetamines
- Adderall
- Memorize these five for the NCLEX
Signs and Symptoms
- Things go UP!
- Euphoria, seizures, restlessness, irritability, hyperreflexia (3+, 4+), tachycardia, increased bowels
- There are over 135 drugs that are downers
- If it is not an upper, it is a downer
Signs and Symptoms
- Things go DOWN!
- Lethargic, respiratory depression/arrest, constipated, etc.
(borborygmi), diarrhea
What are the highest nursing priority to anticipate in an Upper or Downer?
- Upper: The highest priority to anticipate in an Upper is suctioning due to seizures
- Downer: The highest priority to anticipate in a Downer is intubation/ventilation due to
respiratory arrest
Example
One of your pt is “high on cocaine.” What is critically important to assess?
- Having a RR of 12 is not a critical measurement to assess for that pt
- However, assessing for reflexes (3+ or 4+), irritability, borborygmi (increased bowel sounds), or increased temperature would be more appropriate
- The “ABC rule” does not apply here … In fact, the pt’s ABC in cocaine toxicity is unremarkable
After you know that the drug in question is an Upper or a Downer, the second question you should ask yourself is whether it is an Overdose or a Withdrawal
- Overdose and withdrawal have the opposite effects
Overdose
Overdose on an Upper Overdose on a Downer
Too much Too little
Withdrawal
Withdrawal on an Upper Withdrawal on a Downer
Too little Too much
Question
The driver of a squad car calls the ER and says he is bringing a pt who in ODed on cocaine. What do you expect to see? … Select all that apply
- Pt ODed on Upper OD … Expect to se Too much
- First question: Upper or a Downer?
- Second question: Overdose or Withdrawal?
- S/Sx would be: Irritability, 4+ reflexes, borborygmi, increased temperature, etc.
Question
The same pt is withdrawing from cocaine … Same question
- This pt is an Upper in Withdrawal = Too little
- Therefore, respiratory is under 12, pt is difficult to arouse, give them Narcan
Drug Abuse in the Newborn
Always assume intoxication, not withdrawal at birth, in a newborn less than 24 hours after birth. 24 hours or more after birth, you can assume the newborn is in withdrawal
Question
You are caring for an infant born to Quaalude addicted mother 24 hours after birth. Select all that apply
- Overdose/withdrawal condition … Ask the following 2 questions
- Is it an Upper or a Downer? … We don’t what it is because it is a “Quaalude” (it is likely a Downer)
- Is it Overdose or Withdrawal? … 24 hours after birth (Withdrawal)
- A Downer in Withdrawal = Too much
- S/Sx = Difficult to console, seizure risk, shrill, high-pitched cry, exaggerated startle reflex
Alcohol Withdrawal Syndrome vs. Delirium Tremens
Alcohol Withdrawal Syndrome and Delirium Tremens are not the same
- Every alcoholic goes through alcohol withdrawal approximately 24 hours after the person stops drinking
- However, less than 20% of alcoholics in alcohol withdrawal syndrome progress to delirium tremens … Delirium tremens occurs about 72 hours after the person stop drinking
- Alcohol withdrawal syndrome always precedes delirium tremens; however, delirium tremens does not always follow alcohol withdrawal syndrome
Alcohol Withdrawal Syndrome Delirium Tremens
- Occurs after 24 hours after drinking
Non-life threatening to self and others
Nursing Care Plan
- Regular diet
- Semiprivate room, anywhere on the unit
- Pt is up ad lib (Pt is free to move around as desired)
No restraints
- Occurs after 72 hours after drinking
Life threatening to self and others
Nursing Care Plan
- NPO (seizures) or clear liquid diet
- Private room, near nursing station
- Restricted bed rest (Pt is not free to move around as desired—no bathroom)
Restraints (vest or 2-point lock letters)
Note
- “Up ad lib” or “up ad liberum” means pt may have activity or free to move around as desired any time
- 2-point lock letters restraints: Restraints in 1 upper and the contralateral lower extremities. Release and secure upper arm first, and then release and secure the foot. Switch extremities every 2 hours
- Give both anti-HTN medication, tranquilizer, multivitamin containing vit B1
Question
So what two situations would respiratory arrest be a priority?
- Overdose of a Downer
- Withdrawal of an Upper
Question
Which pts would seizure be a risk for?
- Overdose of an Upper
- Withdrawal of a Downers
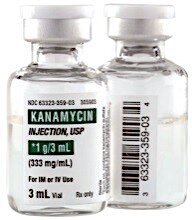
Aminoglycosides (Top 5 most tested drugs)
Aminoglycosides are the big guns of ABXs (antibiotics)— use them when nothing else works. Aminoglycosides are unsafe at toxic levels and safety then becomes an issue. They are the 5th most tested drugs on the NCLEX
The most tested drugs on the NCLEX are:
- Top 5
- Psychiatric
- Insulin
- Anticoagulant
- Digitalis
- Aminoglycosides
- Others
- Steroids
- Beta-blockers
- Calcium channel blockers
- Pain medications
- Obstetrics medications
“A Mean Old Mysin” = Aminoglycosides
Would be used to treat serious, resistant, life-threatening, Gram negatives infections
- So, treat a mean old infection with a “Mean Old Mycin”
- Examples are: TB, septic peritonitis, fulminating pyelonephritis, septic shock, infection from third degree wound covering >80% of the body
- However, sinusitis, otitis media, bladder infection, viral pharyngitis, and strep throat are not old mean infections and are not treated with a mean old mycin
All aminoglycosides end in Mycin
- Gentamycin, Vancomycin, and Clindamycin, Streptomycin, Cleomycin, Tobramycin
- Not all drugs ending in mycin are aminoglycosides
- Azithromycin, Clarithromycin, Erythromycin … All have THRO in the middle … So, THRO them off the “Mean Old Mycin” list
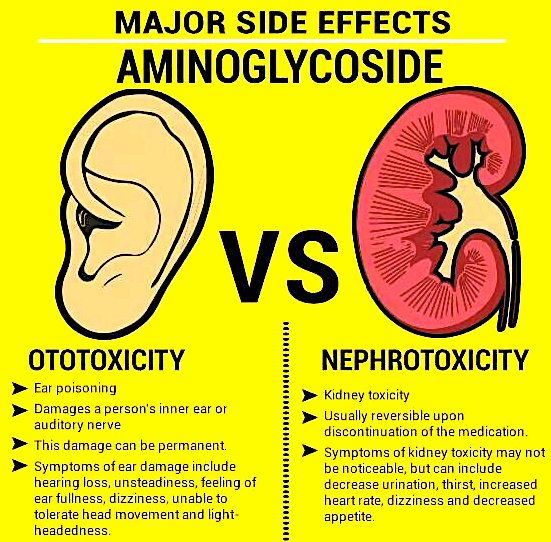
What are toxic effects?
 Mycin—Sounds like Mice (Think ears) … Monitor hearing (#1), balance, tinnitus (ringing of the ear, CN8 toxicity)
Mycin—Sounds like Mice (Think ears) … Monitor hearing (#1), balance, tinnitus (ringing of the ear, CN8 toxicity)- The human ears are shaped like a kidney so another toxic effect of aminoglycosides is nephrotoxicity (Toxic to the kidneys)
- Therefore, monitor Creatinine
What would be your answer if in a question, you have to choose which is the best between 24-hour creatinine and serum creatinine?
- Creatinine = Best indicator of kidney function
- 24-hour creatinine clearance is better than Serum creatinine
The figure 8 drawn inside the ear should remind you of of 2 things They are toxic to CN8
Administer them q8 hour
Do not give Mean Old Mycins PO because they are not absorbed, and therefore would not have any systemic effects
There are 2 cases where Mean Old Mycins are given PO
- Hepatic encephalopathy (or hepatic coma) where ammonia level gets too high
- Pre-op bowel surgery: to sterilize the bowel before surgery
- In both cases, the ABX stays in the gut (not absorbed), sterilizes the bowel, and would not be toxic

The #1 action of an “oral mycin” … Sterilize the bowel
-
- Who can sterilize my bowel?
Neo Kan
-
- Neomycin and Kanamycin
“A Mean Old Mycin” is given IM or IV because it is excreted in feces and not absorbed in the GI tract. It is used in hepatic encephalopathy to kill E. coli, and bowel surgery (to sterilize the bowel).
Note
E. coli in the gut is the #1 producer of ammonia, which at toxic levels, leads to encephalopathy
Troughs and Peaks
- Troughs is when drugs is at their lowest concentration in the pt’s blood
- Peaks is when drugs is at their highest concentration in a pt’s blood
“TAP” Levels
- A method to remember what is done before or after, when dealing with a medication with troughs and peaks
- “TAP”—Trough, Administer, Peak
- Trough before drug administration
- Peak after drug administration
- Trough and Peak levels are drawn because of a drug’s narrow therapeutic window or index
- Narrow therapeutic window or index means that there is a small difference in what works and what kills
Which one of the following medications would “trough and peak” important?
Note
1. Draw TAP on Mean Old Mycins because of their narrow therapeutic index
- Lasix (furosemide)
- Smaller dose: 5 or 10
- Larger dose: 80 or 120
- Digitalis (digoxin)
- Smaller dose: 0.125
- Larger dose: 0.25
- Would draw “TAP” (Trough, Administer, Peak) on digitalis
When to Draw a Through and a Peak
- Both Trough and Peak are not medication-dependent
- The trough, it is always drawn 30 minutes before next dose
- For the peak, it depends on the route
- Peak SubL 5 to 10 minutes after drug is dissolved
- Peak IV 15 to 30 minutes after drug is finished (bag empty)
- Peak IM 30 to 60 minutes
- Peak SubQ Depends on insulin (See diabetes lecture)
- Peak for PO Not necessary, not tested
Question
You give 100 mL of a drug at 200 mL per hour (the drug takes 30 minutes to run). If you hang the drug at 10 a.m., it will finish running at 10:30 a.m. When will the drug peak?
Note
- The same drug given by 2 different routes at the same time will have different peaks
- Morphine
- However, 2 different drugs given at the same time and route (IV) will peak together
- Morphine and amphetamine
1. 10:15 a.m.
2. 10:30 a.m.
3. 10:45 a.m.
4. 11:00 a.m.
Answer: Two right answers—pick 11:00 a.m.
In this case, play the “Price Is Right”—go with the highest time w/o going over
Lecture 3 • Mark Klimek • 111:11
Calcium Channel Blockers
CCBs (Calcium channel blockers) are like Valium for the heart
They relax and slows down the heart
- In other words, CCBs have negative inotropic, chronotropic, dromotropic effects on the heart
(+) Inotropy, Chronotropy, Dromotropy (–) Inotropy, Chronotropy, Dromotropy
Positive inotropy
- Increase cardiac contractile force Ventricles empty more completely Cardiac output improved
Positive chronotropy
- Increase rate of impulse formation at SA
node Accelerate heart rate
Positive dromotropy
- Increase speed that impulses from SA node travel to AV node (increase conduction velocity)
Negative inotropy
- Weaken/decrease the force of myocardial contraction
Negative chronotropy
- Decrease rate of impulse formation at the
SA node decelerate heart rate
Negative dromotropy
- Decrease speed that impulses from SA node travel to AV node (decrease conduction velocity)
When do you want to relax and slows down the heart? … To treat “A, AA, AAA”
- Antihypertensive
- AntiAnginal drugs (decreasing oxygen demand)
- AntiAtrialArrhythmia
Side Effects
Headache and hypotension
Name: ends in “dipine” … Not “pine”
- Also, verapimil, Cardizem (diltiazem)
- Cardizem (diltiazem) is given continuous IV drip
What are the parameters to assess before putting a pt on CCBs?
- Assess for BP
- Hold if SBP <100
Cardiac arrhythmias
- Knowing how to interpret rhythm
- Must know the following 4 cardiac rhythms by sight
Normal Sinus Rhythm
- There is a P wave, followed by a QRS, followed be a T wave for every complex

- Peaks of the P wave is equally distant to the QRS, and fall within 5 small boxes
Ventricular Fibrillation
 No pattern
No pattern
Ventricular Tachycardia

- Sharp peaks with a pattern
Asystole
 A flat line
A flat line
If the question mentions
- QRS depolarization = Ventricular
There are 3 levels of nursing knowledge
- Stuff you need to know
- Stuff that is nice to know
- Stuff that is nuts to know
- P wave = Atrial
The 6 rhythms most tested on the NCLEX
- A lack of QRS complexes is asystole—a flat line
- P waves (atrial) in the form of saw tooth wave = atrial
flutter
- Chaotic P wave patterns = atrial fibrillation (a-fib) (Chaotic: word used to describe fibrillation)
- Chaotic QRS complexes = ventricular fibrillation (v-fib)
- Bizarre QRS complexes = ventricular tachycardia (v-tach) (Bizarre: word used to describe tachycardia)
- Periodic wide bizarre QRS complexes = PVCs (Salvos of PVCs = A short runs of v-tach)
PVCs (premature ventricular contractions) are usually low priority
- However, elevate them to moderate priority if under the following 3 circumstances
- There are 6 or more PVCs in a minute
- More than 6 PVCs in a row
- R on T phenomenon (a PVC falls on a T wave)
- PVCs after an MI is common and is a low priority
Lethal arrhythmias are high priority and will kill a pt in 8 minutes or less. They are:
- Asystole and V-fib (ventricular fibrillation)
- Both rhythms produce low or no cardiac output (CO), without which there is inadequate or no brain perfusion. This may lead to confusion and death
Potentially Lethal Cardiac Arrhythmia
- V-tach (ventricular tachycardia) is a potentially lethal cardiac rhythm but it has a CO
How would a pt with or without CO presents?
- CO is absent = there is no pulse
- CO is present = there is a pulse
Treatment of PVCs and V-tach
- Ventricular = Lidocaine
- Both are ventricular rhythms
- Treat with Lidocaine
- Amiodarone is eventually the NCLEX board will want as answer
Supraventricular arrhythmias are Atrial arrhythmias (supra = above) Treatments are “ABCDs”
- Adenocard (Adenosine) … Fast IV push (push in less than 8 seconds and 20 mL NS flush right after) … These pts will go into asystole for about 30 seconds and out of it
- Beta-blockers (end in -olol)
- CCBs
- Digitalis (digoxin), Lanoxin (another digitalis analog)
Beta-blockers have negative inotropic, chronotropic, dromotropic effects on the heart. They treat “A, AA, AAA”
Tx: Atrial arrhythmias
- Adena
- Beta
- Calcium
- Dig
Tx: Ventricular arrhythmias
- Lidocaine
- Amiodarone
- Antihypertensive
- AntiAnginal drugs (decreasing oxygen demand)
- AntiAtrialArythmia
- Side Effects = Headache and hypotension
Treatment of V-fib and Asystole
- Defib for V-fib (Defib = defibrillate = Shock em!)
- Epinephrine and Atropine for Asystole
Chest Tubes
Purpose: to reestablish negative pressure in the pleural space … Negative pressure in the pleural space makes thing stick so that the lung expands when the chest wall expands
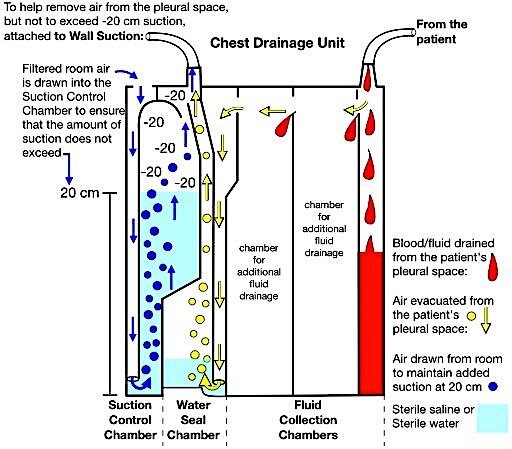
- Pleural space is the space between the lung (visceral pleura) and the chest wall (parietal pleura)
- In a pneumothorax, chest tube removes air
- In a hemothorax, chest tube removes blood
- In a hemopneumo- thorax, chest tube removes air and blood
Question
A chest tube is placed in a pt for a hemothorax (blood). What would you (the LPN) report to the nurse? Or, what would you (the RN) report physician?
-
- Chest tube is not bubbling
- Chest tube drains 800 mL in the first 10 hours
- Chest tube is not draining
- Chest tube is intermittently bubbling
What is the chest tube not supposed to do? The chest tube is supposed to drain instead of bubbling
- Therefore answer (c) is the right answer.
Question
A chest tube is placed in a pt for a pneumothorax (air). What would you (the LPN) report to the nurse? Or, what would you (the RN) report physician?
- Chest tube is not bubbling
- Chest tube drains 800 mL in the first 10 hours
- Chest tube is not draining
- Chest tube is intermittently bubbling
With a pneumothorax, bubbling is expected
- Therefore, (a) is a good answer choice
- Since this is a pneumothorax, not too much blood is expected
- Consequently, 800 mL of blood over 10 hours (80 mL per hour) is too much blood and needs to be reported to the nurse or the physician
Also, pay attention to the location the tube is placed
- Apical (top) or Basilar (base)
- Apical chest tube removes Air
- Basilar chest tube removes
Blood or fluid (due to gravity)
Examples
- An apical chest tube is draining 300 mL the first hour is bad … Bubbling (air) is expected
- A basilar chest tube is draining 200 mL the first hour is expected
- An apical chest tube is not bubbling … This is a bad sign because bubbling (air) is expected
- A basilar chest tube is not bubbling … This is a good sign because bubbling (air) is not expected
Example
Pt presents with a unilateral hemopneumothorax. How to care for this pt?
- Place an apical chest tube for the pneumothorax and a basilar for the hemothorax
Bilateral pneumothorax needs apical chest tube one on the right and one on the left
- Air tube = Apical = Top, on both sides
Posttrauma or postsurgical pt needs
- Pt presents with a unilateral hemopneumothorax. How to care for this pt? … Place an apical and a basilar chest tube on the side of the problem … Always assume trauma and surgery is unilateral unless otherwise specified
Trick question
Were would you place a chest tube for a postop right pneumonectomy?
- Postop right pneumonectomy does not need a chest tube … Since the right lung was removed, there is no need for a chest tube
- Chest tube will however be used for lobectomy (removal of a lobe of the lung), or wedge resection
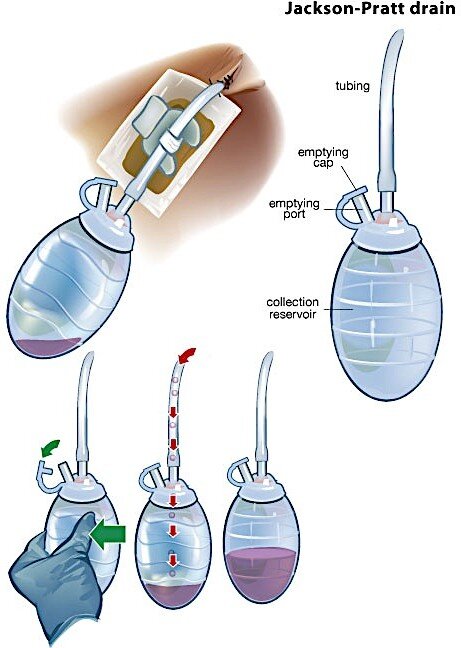
Closed chest drainage devices
Knock someone or something over: to push or strike someone or something, causing the person or the thing to fall
- Types: Jackson-Pratt, Emisson, pneumovac, hemovac, etc.
- What happens if one of those drainage devices is knocked over?
- Ask pt to take a deep breath and set the device back up
- Not a medical emergency … No need to call the physician
If the water seal of the chest tube breaks
- Clamp
- Clamping, unclamping, and placing the tube under water must be done in 15 seconds or less
- Cut the tube away
- Submerge (stick) the end of the tube under sterile water
The most important step
- Unclamp the tube if it was initially clamped, (clamping the tube prevent air to get into the chest but does not allow anything from the chest to get out)
Note
If for whatever reason the chest tube breaks, clamp, unclamping to placing the tube under water must be done in 15 seconds or less
Question
The water seal chamber of the chest tube in a pt with a pneumothorax/hemothorax breaks. What is the first course of action for the nurse?
- Clamp the tube
- Cut the tube away
- Submerge (or stick) the end of the tube under sterile water
- Unclamp the tube if it was initially clamped
In this case, the first course of action is the clamp the tube
Question
The water seal chamber of the chest tube in a pt with a pneumothorax/hemothorax breaks. What is the priority (best) action of the nurse?
- Clamp the tube
- Cut the tube away
- Submerge (or stick) the end of the tube under sterile water
- Unclamp the tube if it was initially clamped
In this question, the priory action for the nurse is to submerge the end of the tube under sterile water because doing so prevents air from getting into the chest. At the same time, this allows air or blood from the chest to get out
- This solves the problem by reestablishing the water seal
Note
Clamping, unclamping, and placing the tube under water must be done in 15 seconds or less
Question
You notice on the monitor that a pt has v-fib. Pt is unresponsive and there is no pulse. What is the first step in the management of this pt?
- Place a backboard under pt’s back while pt is supine
- Start chest compression
The first step is to place the backboard under pt’s back. “First” is about order.
Question
You notice on the monitor that a pt has v-fib. Pt is unresponsive and there is no pulse. What is the best step in the management of this pt?
- Place a backboard under pt’s back while pt is supine
- Start chest compression
“Best” is about what is the priority. Chest compression is the priority action.
If a chest tube gets pulled out …
- Take a gloved hand and cover the opening (first step)
- Take a sterile Vaseline gauze and tape 3 sides (best step)
Chest tube is bubbling … Ask (1) where it is bubbling, and (2) when it is bubbling? Ask the following 2 questions
- Bubbling … Where? In the water seal chamber
- If it is intermittent, it is good (document it)
- If it is continuous, it is bad and indicates a break/leak in the system (find it and tape it)
- Bubbling … Where? In the suction control chamber
- If it is intermittent, suction pressure is too low (increase it at the wall until it is continuous)
- If it is continuous, it is good (document it)
Analogies
- A straight catheter is to a Foley catheter, as a thoracentesis is to a chest tube
- A straight catheter goes in and out … A Foley goes in, secure it, and continuous drainage
- Thoracocentesis = go in and out … Chest tubes = go in, secure it, and leave it in place
- A Foley has a higher risk of infection than a straight cath
- A chest tube has a higher risk of infection than thoracocentesis
Rules for clamping tubes
- Do not clamp a tube for more than 15 seconds without a physician’s order
- Use rubber tooth (will not puncture tubing), double clamps
- Therefore, when the water seal breaks, the nurse has no more than 15 seconds to clamp, cut the tube, submerge it under sterile water, and then unclamp it
Congenital Heart Defects
- It’s either they cause a lot of trouble or no trouble
- But nothing in between
- Memorize one word: “TRouBLe” with the lower case vowels because congenital heart defects are either:
- “TRouBLe” or
- Nothing to worry about
A pediatric pt with “TRouBLe” as congenital heart defect
- Needs surgery now/soon to live
- Has slowed/delayed growth and development (failure to thrive)
- Has a shortened life expectancy
- Parents will experience a lot of grief, financial and emotional stress
- Pt is likely to be discharge home on a cardiac monitor
- After, birth, pt will be in the hospital for weeks
- Pediatrician or pediatric nurse will likely refer pt to a pediatric cardiologist
Question
The nurse is teaching the parent of an infant born with Tetralogy of Fallot. Which of the following should the nurse talked to the parents about in the teaching session?
- The nurse should teach the newborn’s parents all of the choices listed above
A “TRouBLe” congenital heart defect
- “TRouBLe” shunts blood Right to Left
- “TRouBLe” is Blue (cyanotic)
- All “TRouBLe” start with the letter “T”
- Tetralogy of Fallot
- Truncus arteriosus
- Transposition of the great vessels
- Tricuspid atresia
- Totally anomalous of pulmonary vasculature (TAPV)
Except, Left ventricular hypoplastic syndrome
These are examples if No TRouBLe congenital heart defects
- Ventricular septal defect (VSD)
- Patent ductust arteriosus (PDA)
- Patent foramen ovale
- Atrial septal defect
- Pulmonic stenosis
All children with a congenital heart defect, whether TRouBle defect or No TRouBle defect, have
- A Murmur
- An echocardiogram need to be done to find out the cause of the murmur
4 defects of Tetralogy of Fallot — “PROVe”
- Pulmonary artery stenosis
- RVH (right ventricular hypertrophy)
- Overriding aorta
- VSD (ventricular septal defect)
- No need to know what they are … Just need to spot them as answer choices on the board
Infectious Disease and Transmission-Based Precautions
There are 4 transmission-based precautions
- Standard or universal
- Contact
- Droplet
- Airborne precaution
Contact precautions
- Anything enteric (GI, or fecal/oral)
- C. diff., Hepatitis A, E. coli, cholera, dysentery
Staph
- RSV (droplets fall onto object then pt touches object or put it in mouth)
Do not cohort 2 RSV pts unless culture and symptoms say that have the same disease
Herpes
PPE (personal protective equipment) for contact precaution
- Private room is preferred
- Can be in the same room if cohort based on culture and not symptoms
- Hand washing Gown Gloves
- Disposable supply (gloves, paper plates, plastic utensils)
- Dedicated equipment (stethoscope, BP cuff) and toys stay in the room
Droplet precautions
- For bugs travelling on large particles through Coughing, Sneezing to less than 3 feet
- Meningitis
- H. influenza b
- Example: epiglottitis (nothing in the throat)
PPE (Personal Protective Equipment)
- Private room is preferred
- Can be in the same room if cohort based on culture and symptoms
- Hand washing Mask Goggle or Face shield Gloves
- Disposable supply
- Dedicated equipment
Airborne precautions “Air MTV”
- MMR
- TB
- Varicella (chickenpox)
PPE
- Private room is preferred
- Can be in the same room if cohort based on culture and symptoms
- Hand washing Goggle or Face shield Gloves
- Wear mask when living the room
- Keep door closed
- Disposable supply (not essential)
- Dedicated equipment (not essential)
- Negative airflow
PPE (Personal Protective Equipment)
- Order to put in on … The “Gs” are in reverse alphabetical order and “Mask” comes 2nd
- Gown
- Mask
- Goggle
- Gloves
- Order to take it off … Do so in alphabetical order
- Gloves
- Goggle
- Gown
- Mask
Math Problems
Dosage calculation
IV drip rates = Volume × Drop factor / Time
- Micro/Mini drip = 60 drops per mL
- Macro drip = 10 drops per mL Pediatric dose (2.2 lbs = 1 kg)
Lecture 4 • Mark Klimek • 96:58
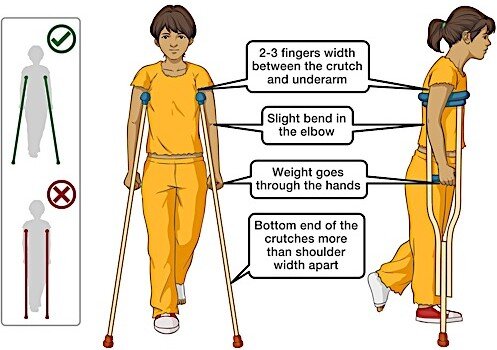
Crutches, Canes, Walkers
One of the major human functions is locomotion. Therefore, crutches, canes and walkers are tested on the NCLEX exam even though they are not really emphasized in school. Also, such knowledge is good for patient teaching. With that said, crutches, canes and walkers are devices used to help pts with an unstable gait, whose muscles are weak or who require a reduction in the load on weight- bearing structures
How do you measure the length of crutches?
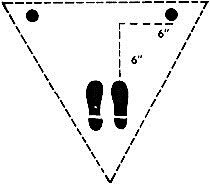 Measuring crutches is important for risk reduction when ambulating and to avoid nerve problems
Measuring crutches is important for risk reduction when ambulating and to avoid nerve problems- The length of a crutch is measured by
- Holding it vertically and placing the tip on the ground
- Having 2 to 3 finger widths between the pad and the
anterior axillary fold
-
- The tip is located to a point lateral (6 inches) and slightly in front of foot (6 inches)
Rule out landmarks on foot or say axilla!
- Handgrip measurement
- The angle of elbow flexion is 30 degrees
- The wrists should be at the level of the handgrip
How to Teach Crutch Gaits?
- point gait—move a crutch and opposite foot together, then the other crutch with other foot together
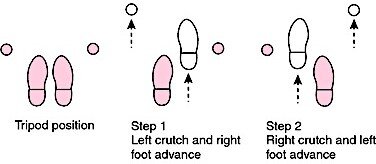
-
- Together (Right leg & Left crutch)
Together (Left leg & Right crutch)
-
- For mild bilateral leg weaknesses
- point gait—move (2 crutches & bad leg) together Followed by unaffected leg
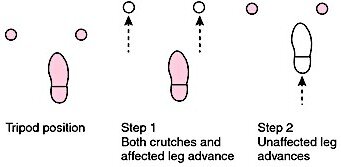
-
- The gait goes 3-1, 3-1, 3-1
- The affected (bad) leg is not on the ground
- The unaffected (good) leg is on the ground
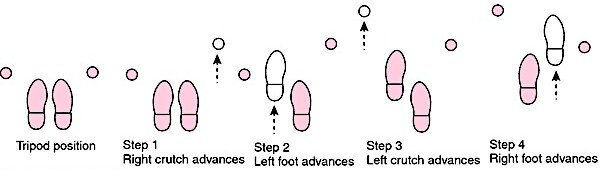
- point gait—move everything separately
- Move crutch Move opposite foot Followed by other crutch Followed by opposite foot
- Right crutch Left foot Left crutch Right foot
- 4-point gait is very slow but very stable
Swing-through is for non-weight bearing (amputees)
-
- Similar to 3-point gait
- The unaffected foot get pass the tip of both crutches
- The person may be an amputee or does not bear weight on the leg at all
- Can move really fast
When do you use these gaits?
-
- Use Even-point gait for even, odd-point gait for odd
- Use the even numbered gaits when weakness in the feet is evenly distributed
- 2-point for mild problems
- 4-point for severe
- Use the odd numbered gait when one leg is affected
- 3-point for one leg
- If pt cannot bear weight or amputation
- Swing-through
Example
A pt affected with early stages of rheumatoid arthritis. What gait should the pt use?
-
- Both legs affected (because it is a systemic disease)
- Early stage—mild
- 2-point gait
Example
A pt has left ATK (above the knee) amputation 2 days ago. What gait should the pt use?
-
- Non-weight bearing
- Swing-through
Example
Pt is first day postop, right knee, partial weight bearing allowed. What gait should the pt use?
-
- One leg affected
- Odd-numbered gait
- 3-point gait
Example
Pt is in advanced stages of ALS. What gait should the pt use?
-
- Bilateral leg weakness (because it is a systemic disease)
- Even-numbered gait
- Advanced stages = Severe
- 4-point gait
Example
Pt with left hip replacement, 2nd day postop on non-weight bearing instruction. What gait should the pt use?
-
- Non-weight bearing of 1 leg
- Swing-through gait
Example
Pt with bilateral (B/L) total knee replacement first day postop. Weight bearing is allowed. What gait should the pt use?
-
- Even-numbered gait = Bilateral
- Weight bearing
- First day postop = Severe
- 4-point gait
Example
Pt with bilateral total knee replacement 3 weeks postop. What gait should the pt use?
-
- Even-numbered gait = Bilateral
- Weight bearing
- 3 weeks postop = mild
- 2-point
Going Up and Down the Stairs With Crutches
-
- Remember this phrase
- “Up with the Good, and Down with the Bad”
- When you go up the stairs, the good foot move up first
- When you go down the stairs, the bad foot move down last
- But, no matter what
- Both crutches always move with the bad leg
- Remember this phrase
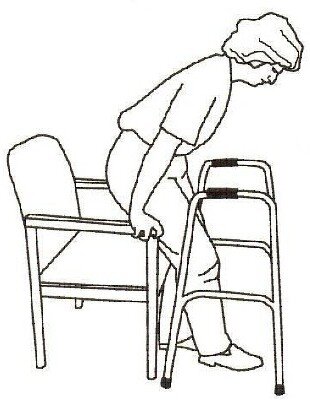
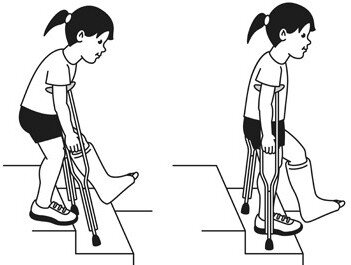
Figure 2. Crutcher.
Figure 3. Cane.
Figure 4. Walker.
Cane
-
- Hold cane on the unaffected (strong) side
- Advance cane with the opposite side for a wide base of support
- Handgrip should be at the level the wrist
Walker
-
- Correct way to use a walker
- The walker is on the side of the pt, the pt “Picks it up … Sets it down … Walks to it”
- Once the walker is in front of the pt, the pt “Holds on to chair, Stands up, Then grabs walker”
- Don’t tie belongings to the front of the walker—Tie them to either side so it won’t tip over
- The NCLEX board does not like tennis balls or wheels on walker can create problem
- Correct way to use a walker
Psychiatry
First thing to ask in a psych question is: “Is the pt psychotic or non-psychotic?”
-
- The answer to this question will determine care plan, treatment, length of stay, legality, etc.
A Non-psychotic person has insight and is reality based. What kinds of answers do you pick for these people? What techniques do you use?
-
- Good therapeutic communication … Looks like a Med/Surge pt
- Examples of therapeutic communications
- That must be very difficult/overwhelming for you
- How are you feeling?
- Tell me more about your …
- The exam is looking for “reflection, clarification, amplification, restatement, etc.”
The Psychotic person has no insight and is not reality based
-
- They don’t think they’re sick—everyone else has the problem
- Examples are: delusions, hallucinations, illusions
- They don’t think they’re sick—everyone else has the problem
Delusions, hallucination and illusion are psychotic symptoms

-
- Delusions—a false, fixed belief or idea or thought. There is no sensory component. It is all in your head. It is just a thought … 3 types of delusion
- Paranoid—People are out to get/kill me
- Grandiose—“I’m Christ” … “I am the President” … “I am the world’s smartest person”
- Somatic—Body part (I have x-ray vision, there are worms inside my arm)
- Hallucination—a sensory experience
- Auditory (1st m c)—voices telling you to harm yourself
- Visual (2nd m c)—I see bugs on the wall
- Tactile (3rd m c)—I feel bugs on my arm (Most common = m c)
- Gustatory (taste)
- Olfactory (smell)
- Illusion—a misinterpretation of reality. It is sensory
- Delusions—a false, fixed belief or idea or thought. There is no sensory component. It is all in your head. It is just a thought … 3 types of delusion
Differentiation between hallucination and illusion
-
- With illusion there is a referent in reality
- A referent is something that both the clinician and the pt can refer to … There is actually something there
- The cord is a snake
- With hallucination, there is nothing there
- With illusion there is a referent in reality
Example
The pt staring at the empty wall says, “Listen, I hear demon voices.” Is that statement from the pt a hallucination and an illusion?
-
- There is no referent there
- This is a hallucination
Example
The same pt overhears nurses and doctors laughing and talking at the nursing station, and says, “I hear demon voices.” Is that statement from the pt a hallucination and an illusion?
-
- There is actually a referent (real people) there
- This is an illusion
Other examples
-
- A pt looks with a blank stare and says, “I see a bomb.”
- This is a hallucination
- A pt looking at the fire extinguisher on the wall and says look, “I see a bomb.”
- This is an illusion
- A pt looks with a blank stare and says, “I see a bomb.”
How do you deal with these psychotic patients?
-
- To deal with these psychotic pt, the first thing to ask is what type of psychosis the pt has?
There are 3 types of psychosis
- Functional psychosis
- Psychosis of dementia
- Psychosis of delirium
- Functional psychosis—they can function in everyday life
- 90% of the followings make up this category
- Chemical imbalance in the brain
- They are “Skeezo, Skeezo, Major, Manics”
o Schizophrenia, Schizoaffective disorder, Major depression (not depression), Mania
Example
- Bipolar = Depression and Mania
- Bipolar pts are psychotic in acute mania
- Psychosis of dementia—what is their problem?
- Actual Brain destruction/damage
- Due to Alzheimer, stroke, organic brain syndrome
- Anything that says Senile/Dementia falls in the category
- Psychotic Delirium—temporary, sudden, dramatic, episodic secondary to something else
- Loss of reality
- Due to UTI, thyroid imbalance, adrenal crisis, electrolytes, medications/drugs
Recap
Approach to Answering Psychiatric Questions
- First thing to ask is
- Is the pt non-psychotic? Or, is the pt psychotic?
- Pt is non-psychotic
- Address pt as you would address any Med/Surg pts Use therapeutic communication
- Pt is psychotic
- Next, ask if they are functional, demented, or delirious?
Functional = (1) Acknowledge feeling, (2) Present reality, (3) Set limits, and (4) Enforce these limits
Demented = (1) Acknowledge their feeling, and (2) Redirect them—give them something they can do
Delirious = (1) Acknowledge feeling, (2) Reassurance about safety and temporariness of their condition
Functional Psychosis
- Schizo, mood disorders thought process, and mania (chemicals out of whack)
- This pt has the potential to learn reality (no brain damage)
- Your role as a nurse—teach reality
- Use the 4 step process to teach reality
- (1) Acknowledge feeling, (2) Present reality, (3) Set limits, and (4) Enforce these limits
What does this look like in a question?
-
- The answer acknowledges pt’s feeling (look for the word “feel”)
You seem upset … That is so sad … It’s been so difficult … Tell me more about how you’re feeling
-
- Now, present reality … “I know you see that demon, but I don’t see a demon” … Or, “I am a nurse, this is hospital, this is your breakfast”
- Set limit. ”We are not going to address that. Stop talking about…”
- Enforce limit. “I see you’re too ill, so our conversation is over.” Ends the conversation. You’re not punishing the client by taking away privileges
Psychosis of dementia
- They cannot learn reality … Don’t present it! They can’t learn it! Thus frustrates them, and may discourage you!
- Deal with their problems in 2 steps
- (1) Acknowledge their feeling, and (2) Redirect them—give them something they can do
Do not confuse not presenting reality with reality orientation (Person, place, and time)
- Reality orientation = Pt is oriented to person, place, and time
Example
- Alzheimer lady is the lobby of waiting area of her nursing home. It is Sunday and she is all dressed up. You day to her, “Mrs. Smith, you are all dressed up.” She said, “Yeah! My husband is going to pick me up. We are going to church.” The problem is that the husband has been dead for 10 years.
- She has a false, fixed belief
- She is delusional (or she is psychotic)
- What do you say to her?
- First, acknowledge her … You say, “That sounds nice.” (acknowledging)
- Second, redirect her … You say, “Why don’t we sit down here and talk about church? … What church do you go to?” (redirecting)
- Don’t tell her husband is dead!, which is presenting reality
Psychosis of delirium
- This is temporary, sudden, dramatic, episodic, secondary loss to reality
- Usually due to some chemical imbalance in the body
- Causes—UTI, thyroid imbalance, adrenal crisis, electrolytes, medications/drugs
- To manage these pts, treat the underlying cause
- Acknowledge feeling
- Reassure them of safety and temporariness of their condition
- They lost touch with of reality—Redirect them is futile
Example
A pt with schizoaffective disorder who points to 2 people talking across the room. The pt says, “Those people are plotting to kill me.” What would you say? What is the most important word in the vignette?
- Schizoaffective—psychosis
- I can see that would be frightening. They are not plotting.
- We are not going to talk about that. I can see you are too ill. We are ending the conversation
Example
A pt with Alzheimer disease who during your conversation points to 2 people talking across the room and says, “You see these people, they are plotting to kill me”
- Alzheimer Disease—category is dementia
- Acknowledge feeling—“I understand you seem to be scared”
- Redirect—Let’s go somewhere you feel safe
Example
A pt with delirium tremens who during your conversation points to 2 people talking across the room and says, “You see these people, they are plotting to kill me”
Delirium tremens …
- “That must be scary”
- But you are safe. Your fear will go away when you get better
Psychotic symptoms
Loose associations

- Flight of Ideas: Rapid flow of though
- Word Salad: Throw words together and toss out … (Sicker than flight of ideas)
- Neologisms: Make it up
- Narrowed self-concept: When a psychotic refuse to change their clothes or leave the room. Leave them alone
- This is a functional psychosis
“Don’t make a psychotic do something they don’t want to do”
- Idea of reference: You think everyone is talking about you
Dementia hallmark: Memory loss, inability to learn
- Always acknowledge feeling
- 2nd step always begins with “Re” … Reassure, Redirect, Reality
Recap
Approach to Answering Psychiatric Questions
- First thing to ask is
- Is the pt non-psychotic? Or, is the pt psychotic?
- Pt is non-psychotic
- Address pt as you would address any Med/Surg pts Use therapeutic communication
- Pt is psychotic
- Next, ask if they are functional, demented, or delirious?
Functional = (1) Acknowledge feeling, (2) Present reality, (3) Set limits, and (4) Enforce these limits
Demented = (1) Acknowledge their feeling, and (2) Redirect them—give them something they can do
Delirious = (1) Acknowledge feeling, (2) Reassurance about safety and temporariness
of their condition
Lecture 5 • Mark Klimek • 71:46
Diabetes Mellitus (DM), Diabetes Insipidus (DI), Insulin
Diabetes mellitus = An error in glucose metabolism … Glucose is the body’s primary fuel source
- Can be a lack of insulin DM1
- Can be insulin resistance DM2
DIABETES INSIPIDUS = Not a type of DM! … It is insidious, diabetes w/out the glucose element
- It is Polyuria, Polydipsia leading to dehydration, due to low ADH.
- It is just the fluid part
So question is about low urine output or high urine output? …
- Similar to DM, DI has a high urine output
What is the opposite of Diabetes Insipidus?
- It is SIADH = Syndrome of inappropriate ADH (antidiuretic hormone)
So, DM has polyuria, polydipsia Therefore, DI also has polyuria, polydipsia
However, SIADH is the opposite of the above 2 conditions …
- It presents w/ oliguria and no thirst
- Decrease urine output
- And then, decrease serum specific gravity (due to retention of water)
- Increase urine specific gravity (due to decrease urine volume)
Lots of urine retained, specific gravity is low = SIADH Fluid Volume Deficit = DM, DI
Nursing Diagnosis?
Fluid Volume Excess = SIADH
Diabetes
- Type I—Insulin dependent, Juvenile onset, Ketosis prone
- Type II—Non-insulin dependent, Adult onset, Non-ketosis prone
- S/Sx of DM
- Polyuria—pee a lot
- Polydipsia—thirsty
- Polyphagia—(eat/swallow a lot)
Treatment for DM Type I (if you don’t treat)
- They will “DIE”
- Diet (calories from carbs, least important)
- Insulin (most important)
- Exercise
Treatment for Type II DM
- They are “DOA”
- Diet (most important)
- Oral hypoglycemic
- Activity
Diet for DM2
- Primary treatment modality is Calorie restriction
- 1200 Cal, 1400 Cal, 1600 Cal
- These pts need to eat 6 small feeding per day—smaller more frequent meals—keeps blood sugar more stable
Question
What is the best dietary action a DM2 should take?
-
-
- Restrict calories
- Divide meal into 6 feedings a day
-
Answer: (a) because pt can eat 6 meals but does not limit the Cal with each meal Insulin acts to lower blood sugar
4 types of Insulin are covered here
R-Regular insulin—clear solution, IV drip (HESI-intermediate, Rapid, Run IV)
-
- Onset: 1 hour
- Peak: 2 hours
- Duration: 4 hours … (Audio says 3 hours, but it is 4 hours)
- Pattern: 1-2-4 (Pay attention to peak)
N-NPH, Intermediate insulin—it is cloudy, N = Not So Clear, Fast (Cloudy = Suspension—it precipitates—can’t give IV drip), N = not so fast, not in the bag
-
- Onset: 6 hours
- Peak: 8 to 10 hours
- Duration: 12 hours
- Pattern: 6-8-10-12 (Hear the even #s and pay attention to peak)
Clear = Solution
Cloudy = Suspension Will precipitate (Not given over IV drip or put in an IV bag)
Question
How would the board ask question about peak of insulin?
For instance, you give 30 units of insulin to a pt at 7 a.m. When do you check for hypoglycemia?
-
- Answer = Add the insulin peak time to the time of insulin administration
- For instance, if the pt was given NPH at 7 a.m., add 8 to 10 hours to the time
- Answer = Check for hypoglycemia between 3 and 5 p.m.
Lispro: (Humalog)
-
- Don’t give it AC (before meal) … Give it with the meal
- Onset: 15 min
- Peak: 30 min
- Duration: 3 hrs
- Pattern: 15-30-3
Glargine (Lantus)
-
- Long-acting insulin
- No Peak
- Duration 12 to 24 hrs
- Little to no risk for hypoglycemia (only one you can safely give at bedtime)
Note: Always check insulin expiration date What action invalidates the manufacturers date?
-
- Opening the package
- Once the package is open, the new expiration date is 30 days after that
- Open package without an opening or expiration date should be thrown out
- Label the package either with
- “OPEN” and date package is open or
- “EXP” and expiration date
- Once the package is open, refrigeration is optional
- However, unopened bottle must be kept refrigerated
- Although it is good practice to teach pt to refrigerate insulin at home
Exercise potentiates insulin action
-
- Exercise is like another shot of insulin
- Therefore, if a student is schedule to play soccer (exercise) this afternoon … It is necessary to decrease the dosage of insulin
- In addition, the school nurse must give the student rapidly metabolized carbohydrates— snacks or juice
Sick Days … Pt has a fever or the flu, and so on
-
- Serum glucose levels go up
- Need their insulin even though pt is eating
- Take sips of water because they get dehydrated
- Any sick diabetic pt has 2 problems
- Hyperglycemia and Dehydration
Acute complications of Diabetes
-
- Low blood glucose—a.k.a. Hypoglycemia or Hypoglycemic shock or Insulin shock/reaction
- Why are some of the causes
- Not enough food
- Too much insulin (#1 cause, can lead to permanent brain damage)
- Too much exercise
What does hypoglycemia look like?
-
- Think of Drunk pt in Shock
- Drunk
- Staggering gait
- Slurred speech
- Cerebral impairment (labile)
- Slow reaction time
- Decrease social inhibition
- Shock—Vasomotor collapse
- Tachycardia, tachypnea, Low BP
- Cold/clammy, mottled skin
Treatment
-
- Give pt sugars or Rapidly metabolizable carbohydrate such as
- Juice (any), candy, regular soda, milk (lactose), honey, icing, jelly, jam
- Boards want sugar + starch or protein
- For example, apple juice + turkey, Milk is sugar/protein—1/2 cup Skim milk
- Bad answer
- Candy + Soda—1 sugar is good, 2 sugars are bad
- 5 packs of sugar emptied into a glass of orange juice
- Unconscious pts—pay attention to location
- Glucagon IM if the mother is on the phone
- Dextrose IV (D10, D50) if in the ER
- Give pt sugars or Rapidly metabolizable carbohydrate such as
DKA—High Glucose in a Type I (keto is the clue!)
Causes
-
- Too much food
- Not enough insulin
- Not enough exercise
#1 cause acute viral Upper Respiratory Infection within last 2 weeks
S/Sx of DKA is “DKA”
-
- Dehydration (dry, poor skin elasticity and turgor, warm) … Water is a coolant (you overheat)
- Ketones in serum, Kussmauls, High K+
- Acidosis, Acetone breath, Anorexia due to nausea
Note: Ketone in urine does not necessarily means DKA
Treatment
-
- Insulin IV (Regular!)
- IV fluid! 200 mL/hr (some of the fastest rate)
HHNK or HHS or HHNS
-
- High blood sugar in a Type 2
- These pts don’t burn ketones, no acid
- Whenever you see HHNK, think dehydration
- Severe Dehydration!
- Skin is dry, flushed, decreased turgor, increased HR
- #1 Nursing diagnosis: fluid volume deficit (same as dehydration)
- #1 Nursing intervention: Rehydration!
- Outcomes in successful treatment: Increase urine output, Moist mucous membrane, etc.
- Long-term complications: Poor perfusion, Peripheral neuropathy
Between DKA and HHNK
-
- Which one is more dependent on insulin?
- DKA pt is more dependent on insulin
- HHNK pt needs to be rehydrated
- Which one has a higher mortality rate?
- More pts die HHNK
- Which is a higher priority?
- DKA is a more acute condition and responds very quickly to insulin
- HHN pts show up late in the emergency room and do not readily respond to treatment
- Which one is more dependent on insulin?
Long-term complication of diabetes
-
- Related to
- Poor tissue perfusion or
- Peripheral neuropathy
- Examples of long-term complications: Renal failure, Gangrene, Heart failure, Urinary incontinence, Pt can’t feel a burn on the foot
- For instance
- Renal failure is a cause of poor perfusion
- Urinary incontinence is a cause of peripheral neuropathy
- Related to
Which lab test is the best indicator of long-term blood glucose level?
-
- Hb A1C, a.k.a. glycosated Hb or glycosylated Hb
- Average blood sugar over last 90 days
- (Hb = Hemoglobin)
- Hb < 6 is normal
- Hb > 8 is out of control
- Hb 7 Borderline—have pt come in for evaluation
- Hb A1C, a.k.a. glycosated Hb or glycosylated Hb
Lecture 6 • Mark Klimek • 87:50
Drug Toxicities, Hiatal hernia, Dumping syndrome Drug Toxicities—Know these FIVE medications
- Lithium (antimania drug)
- Used for Bipolar
- Specifically, for the manic episodes but not for the depression
- Therapeutic level: 0.6 to 1.2
- Toxic level: >2.0
- Notice gray area: 1.3 to 2
- Used for Bipolar
Lanoxin or Digoxin
-
- Used to treat A-Fib and CHF
- Therapeutic level: 1 to 2
- Toxic level: >2

- Aminophylline—muscle spasm relaxer for the airway
- Compound of the bronchodilator theophylline
- Therapeutic level: 10 to 20
- Toxic level: >20
- Non-therapeutic level: <10 … if it is not therapeutic, increase dose of medication, and assess for compliance
Dilantin (phenytoin)
-
- Seizure medication
- Therapeutic level: 10-20
- Toxic level: >20
Bilirubin
-
- Breakdown product of Red Blood Cells
- Normal level in adults: 0.2 to 1.2
- Always tested in the Newborns on the NCLEX
- In Newborns bilirubin is much higher than in adults
- Elevated level: 10 to 20
- Toxicity: >20
- When do physicians want to hospitalize these newborns?
- When bilirubin level is about 14 to 15
Patterns
-
- 1s and 10s
- 2s and 20s
- 2s: Low # (Lithium and Lanoxin)
- 20s: High # (Aminophylline, Dilantin and Bilirubin)
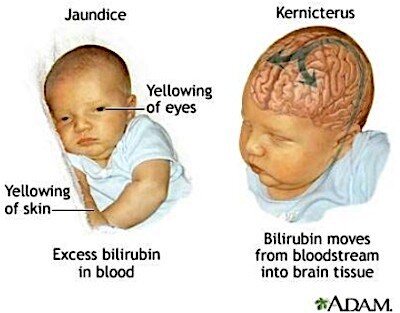
Jaundice—Yellow skin from excess bilirubin in the blood
-
- It appears as yellow skin and sclera
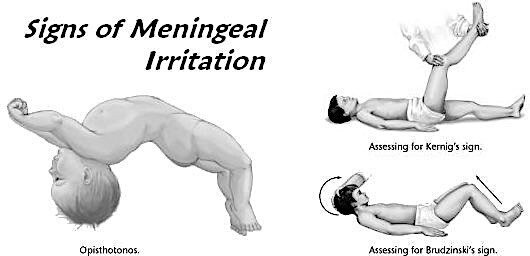
Kernicterus—Excess bilirubin in the brain
-
- Occurs when level in the blood gets >20
- In the brain, it may cause aseptic (sterile) meningitis or encephalopathy (don’t need to know)
- It can be DEADLY
Opisthotonos
-
- Position the newborn assume due to irritation of the meninges from kernicterus
- Presentation: hyperextended posture … (Is a medical emergency)
Question
In what position do you place an opisthotonic newborn?
-
- Put newborn on the side
Pathological vs. Physiological Jaundice
-
- If the newborn comes out yellow, something is wrong = Pathologic jaundice
- If the newborn turn yellow 2 to 3 days postpartum, that’s ok = Physiologic jaundice
Dumping Syndrome vs. Hiatal Hernia
-
- Both gastric emptying problems and are opposites
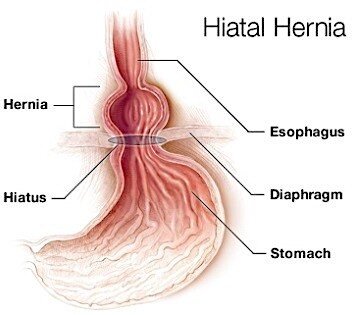
Hiatal Hernia
-
- Regurgitation of gastric acid upward or backward into esophagus
- “Like a cow with 2 stomachs,” gastric contents go in wrong direction at the correct rate
- S/Sx of hiatal hernia is similar to GERD (Heartburn and indigestion)
- S/Sx of hiatal hernia = S/Sx of GERD when lying down after a meal
- In other words, Heartburn, Indigestion on lying down after eating
Treatment
-
-
- Can do 3 things, as shown below
-
- Elevate HOB (head of bed) during and 1 hour after meals
- Increase the amount of fluids with meals
- Increase the amount of Carb content
-
-
- These cause the stomach to empty quickly so its content doesn’t back up
- High-atal Hernia … Everything high
-
-

Dumping Syndrome
-
- Gastric contents are dumped too quickly into duodenum
- Right direction but at wrong rate
- S/Sx of dumping syndrome
- Drunk: Staggering gate, impaired judgment, labile—all blood gone to gut
- Also get Shock: cold/clammy, tachycardia, pale
- Now add Acute abdominal distress: n/v, diarrhea, cramping, guarding, borborygmi, bloating, distention
- Dumping syndrome = Drunk, Shock, Acute Abdominal Distress
- Gastric contents are dumped too quickly into duodenum
Note
-
- Drunk is what it is
- Shock is what it is
- Drunk + Shock = Hypoglycemia
- Drunk + Shock + Acute abdominal distress = Dumping syndrome
Treatment of Dumping Syndrome
-
- Can do 3 things, as shown below
- Lower HOB (head of bed) during meals and turn pt on the side
- Decrease the amount of fluids 1 or 2 hours before or after meals
- Decrease the amount of Carb content
-
- These 3 things prevent the stomach to empty quickly or dump its content into the duodenum
- Dumping syndrome … Everything low
-
What is protein is added in the diet?
-
- Protein does the opposite of carbohydrate
- Protein bulks gastric content, takes longer to digest, and moves slower through the gut
- Therefore, give
- Low protein in hiatal hernia
- High protein for dumping syndrome
Electrolytes
-
- Memorize these 3 sentences
- Kalemias do the same as the prefix (hypo-, hyper-), except for HR and urine output which go opposite
- Calcemias do the opposite as the prefix
- Magnesemias do the opposite as the prefix
- Natremias
- HypoNatremia = Volume overload … HyperNatremia = Dehydration
- Natremias
Kalemia(s)
-
- Go in the same direction as the prefix, except for HR and urine output (UO), which go in the opposite direction
- Hypo—Symptoms go low with hypo, except HR and UO
- Hyper—Symptoms go high with hyper, except HR and UO
Some S/Sx of Hyperkalemia
-
- Brain: seizures, agitation, irritability, loud down
- Heart: tented T waves, ST elevated, tachypnea
- Bowel: diarrhea, borborygmi
- Muscle: spasticity, increase tone, hyperreflexia (3+, 4+)
- Heart rate: down (bradycardia)
- UO: down (oligouria)
Some S/Sx of Hypokalemia
-
- Lethargy, bradypnea, paralytic ileus, constipation, muscle flaccidity, hyporeflexia (0, 1+)
- Tachycardia (HR is up)
- Polyuria (UO is up)
Question
Your patient has hyperkalemia, select all that apply
- Adynamic ileus
- Obtunded
- 1+ reflex
- Clonus (irritable)
- U wave
- Depressed ST
- Polyuria
- Bradycardia
Answer
-
- Kalemia goes in the same direction, except HR and urine output … therefore,
- Clonus are bradycardia are right
Calcemia(s)
-
- Go in the opposite direction as the prefix
- Hypo—Symptoms go high with hypo
- Hyper—Symptoms go low with hyper
Calcemias do the opposite of the prefix—it is a sedative
-
- So Hypercalcemia is bradycardia, bradypnea, flaccid, hypoactive reflexes, lethargy, constipation, etc.
- So Hypocalcemia is agitation, irritability, 3+ or 4+ reflexes, spasm, seizure, tachycardia, Chvostek sign (tap the cheek), Trousseau (inflate BP cuff), etc.
Choosing answers for potassium and calcium
-
- For potassium pick answers related to heart problems
- For calcium pick answers related to muscle problems
Magnesemia(s)
-
- Magnesium goes in the opposite direction of the prefix—it is also a sedative
It is possible that S/Sx are from several electrolytes imbalances. In that case,
-
- Choose CALCIUM if nerve or skeletal involvement
- Pick POTASSIUM for any other symptom
- Generally anything effecting blood pressure
Your patient has diarrhea … Which one of the following electrolyte imbalances causes diarrhea?
Hyperkalemia, hypokalemia, hypocalcemia, or hypomagnesemia
-
- Tetany? Hypocalcemia
Test tip
-
- Common mistake
- Tetany = Hyperkalemia—prefix example. Pay attention
Natremia(s)—Sodium
-
- HypErnatrema = DEhydration
- Hot, flushed, dry skin, thready pulse, rapid HR … Give fluid
- Associate “E” in hypernatremia with DEhydration
- HypOnatremia = Overload
- Crackles, distended neck veins … Fluid restriction, Lasix
- Associate “O” in hyponatremia with Overload
- Nursing Dx: Fluid Volume Excess
- HypErnatrema = DEhydration
Question
In addition to a high potassium, what other electrolyte abnormality can be seen in DKA?
-
- Hypernatremia = Dehydration
- DKA should make you think of DEhydration, which is also associates with hypErnatremia
Question
In addition to High Potassium what other electrolyte imbalance is possible in DKA?
-
- Answer: Hypernatremia
Review—Think dehydration or Fluid overload
-
- SIADH: Hyponatremia
- DI: Hypernatremia
- HHNK: Hypernatremia
How to spot early signs of electrolyte imbalance?
-
- The earliest sign of any electrolyte disturbance is
- Numbness and tingling = Paresthesia
- Circumoral paresthesia = Numbness and tingling around the lips
- The earliest sign of any electrolyte disturbance is
The universal sign of all electrolyte imbalances is
-
-
- Muscle weakness = Paresis
-
Treatment
-
- Potassium is the only one Boards will test
Never Push Potassium IV
-
- Potassium <40 mEq/L of IV fluid
- If >40 mEq/L, clarify dosage with physician
- Potassium <40 mEq/L of IV fluid
How do you lower potassium?
-
- Of all electrolyte imbalance, high potassium is the most problematic
- High potassium can stop the heart
- The fastest way to lower potassium level is to
- Give D5W and regular insulin to decrease potassium
- This will drive the potassium into the cell and out of the blood
- Temporary solution but quick
- Kayexalate is long-term solution
- Through enema or ingestion, Kayexalate exchanges potassium for sodium
- Potassium is eliminated through feces and pt becomes hypernatremic
- Hypernatremia is managed with IV fluid administration
- The downside is it takes hours to work
- To solve this problem
- Give D5W, Regular insulin, and Kayexalate and the same time D5W and Regular insulin work instantly
Kayexalate works in a few hours—K Exits Late
Lecture 7 • Mark Klimek • 115:33
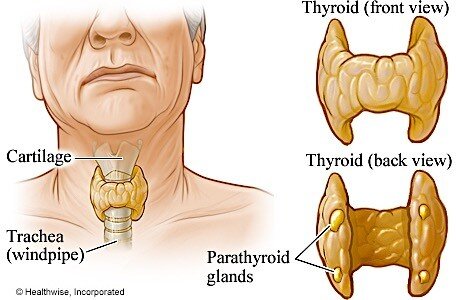
Thyroid and Adrenals
Since the thyroid gland regulate metabolism, whenever you see the word “thyroid,” change it to
“metabolism”
Hyperthyroidism
-
- Hypermetabolism
-
- So, what are the S/Sx of hypermetabolism?
- Weight loss
- HR up, BP up
- Hyperpersonality
- They have heat intolerance … Can tolerate cold because body is like a furnace
- Exophthalmos (bulging eyes) … Think Susan Sarandon, or Don Knotts
- So, what are the S/Sx of hypermetabolism?
Exophthalmos is seen in Graves disease Run yourself into the Graves disease
Hyperthyroidism—3 Treatment Modalities
- Nuke it with radioactive iodine
- Pt must flush three times after urinating
- Call hazmat team if urine is spilled on the floor
- Pt needs a private room in the first 24 hours
- Visitors restriction and in hospital and at home in first 24 hours
- PTU (Propylthiouracil)
PTU “Puts Thyroid Under”
Figure 5. Don Knotts with Exophthalmos or bulging eyes.
-
- PTU’s primary use is for cancer—Monitor WBC b/c pt is immunosuppress
- Thyroidectomy
- Surgical removal of the thyroid is the
most common treatment
-
- To answer questions on the Board correctly, pay attention whether it is a Total, Sub (a.k.a. Partial) thyroidectomy
- Total thyroidectomy needs lifelong hormone replacement, and pt is risk for hypocalcemia due to difficulty to spare the parathyroid glands
Question
What are the symptoms of hypocalcemia?
-
- Paresthesia, tetany, twitching, spasm, clonus, seizure, jitteriness, tremor (all UP!). also, Chvostek and Trousseau signs
Treatment of Subthyroidectomy
-
- Do not need lifelong hormone replacement
- May need to supplement at first
- HOWEVER, they are at risk for thyroid storm
S/Sx of thyroid storm — A medical emergency
-
- Temps of 105 or above
- Get temp down, bring oxygen up
- Bring body temperature down using ice packs/cooling blankets
- Oxygen per mask at 10L
- Stay with patient
- High BP, stroke level — about 210/180
- Severe tachycardia 180 as high as 200
- Psychotically delirious
- Temps of 105 or above
Lowering body temperature in thyroid storm
-
- First step is ice pack
- Best step is cooling blanket
Postop Risks in total thyroidectomy and subtotal thyroidectomy
-
- First 12 hours—risks are the same for both total and subtotal
- Top priority is airway, due to edema
- Next is hemorrhage because it is an endocrine gland—very vascular
- Next 12 to 48 hours—It matters what kind of surgery you’ve had now
- Total: big danger is tetany due to low calcium
TOTAL = TETANY … Can close off airway with an irreversible spasm
- Subtotal: big danger is thyroid storm
SUBTOTAL = STORM (Severe)
-
- After 48 hours—risk is infection
Note: For any type of procedure, the risk of infection significantly increases after 72 hours
Hypothyroidism
-
- Hypometabolism
- So, what are the S/Sx of hypomatabolism?
- Obesity
- HR down, BP down
- Personality: Flat, boring, dull
- They have cold intolerance … Can tolerate heat
- Academically challenged
Myxedema
-
- This is when a pt with severe hypothyroidism presents with skin involvement
Myxedema coma
-
- Severe hypothyroidism leading to decreased mental status, hypothermia, and other symptoms related to slowing of function in multiple organs
- Medical emergency
Treatment of hypothyroidism
-
- Levothyroxine (Synthroid)
- Taken in the morning 30 minutes to 1 hour before breakfast
- Taken alone on an empty stomach with water
Do not sedate these pts
-
- They’re already super slow. They can go into a coma
Question
What pre-op order from the physician would you question?
-
- Ambien (zolpidem) at hs
- (at hs = at bedtime)
Question
A pt dx with hypothyroidism will be undergoing surgery the next morning. The physician ordered the pt NPO at 12:00 am. Pt is on Synthroid and multivitamin pills. What should the nurse question?
-
- Clarify the NPO order for the Synthroid … Why?
- The pt needs the Syntroid medication to get through surgery. Otherwise, the condition may potentiate the suppressing effects of the anesthesia during surgery
- Therefore, don’t hold thyroid pills unless explicitly orders
- Clarify the NPO order for the Synthroid … Why?
Adrenal Cortex Disease
Interestingly, all adrenal cortex diseases either start with an “A” or a “C”
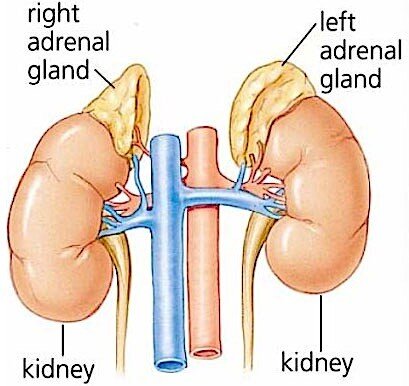
-
- Addison Disease (a.k.a. hypoadrenalism or adrenal insufficiency), Cushing
Addison disease
-
- Under secretion of steroids (they are a time bomb!)
- S/Sx: pts are Hyperpigmented (very tan)
- They do NOT adapt to stress
Question
What is the purpose of the stress response in an individual?
-
- To maintain
- A normal blood pressure to perfuse the brain and other organs
- An adequate level of glucose to feed the body
- To maintain
Question
What could happen if these pts can’t adapt to stress?

-
- Under stress, pts with Addisson disease will go into shock and have an hypoglycemic episode (Addisonian crisis)
Treatment
-
- Give steroids
- Glucocorticoids drugs that end in -SONE
- Prednisone
- Methylprednisone
- “In Addison, you ADD-a-SONE”
Cushings Syndrome
-
- If you have a cushy touchie … You got more
- Oversecretion of adrenal cortex (steroids)
All the S/Sx of Cushings are the S/E of Steroid medications
-
- Draw picture of a little man
- Give man a MOON FACE
- Give him a beard—hirsutism
- Draw a big body—truncal or central obesity
- Arms and legs are skinny—muscle atrophy
- Bump on front—gynecomastia (big breast)
- Bump on back—buffalo hump
- Fill him full of water (he is retaining Na+ and water) He is losing K+ out the back
- Give him some striae—stretch marks
Most important one of all—high serum glucose
-
-
- Do Accu-Checks q6h. They look like diabetics
- Easy bruising—put bruises all over him
- Make him say something in a speech balloon … “I’M MAD, BECAUSE I HAVE AN INFECTION”
- Grouchy (“Roid rage”)
- Immunosuppressed
-
Figure 6. Cushings disease.
Important! … Draw this picture over and over, while repeating the list on the left such that to commit to memory the S/Sx of Cushings and the S/E of steroid medications
Question
A pt comes in with an acute exacerbation of COPD. The pt is being treated with Solu-Medrol (methylprednilosone) IV push q8 hours to reduce the inflammation in the airway. What nursing action needs to be taken while the pt is on the medication?
-
- Do an Accu-Checks q6 hours
- Since pt is on steroid, his condition is similar to diabetes even though he is not diabetics
- The complications are worse if pt is diabetic
Treatment for Cushings
-
- Adrenalectomy
- What happens with a bilateral adrenalectomy?
- Now pt has Addison disease
- Now give steroids (ending in SONE) to treat.
- Pt will start looking like Cushman (Cushinoid-like)
- It takes about a year or so—after a lot of titration—for the pt to start looking normal
Kids Toys (50:16)
When you select toys and play activities for children, there are three things to consider
- Is it safe?
- Is it age appropriate?
- Is it feasible?
- Is it possible to do easily or conveniently?
- For instance, swimming in hospital with body cast
Safety
-
- Size (no small toys for kids under 4)
- Over 4 small pieces are fine
- NO Metal (or dye-cast) if oxygen is in use
- Think of a flint-sparks!
- Beware of fomites
- A fomite is a non-living object that harbors microorganisms, such as stuffed animals—the worst type of fomites
- Hard plastic toys are fine … They can easily be disinfected
Note
If you have a child who is immunosuppressed … Give them a hard plastic action figure. It can easily be disinfected
Age appropriate toys (See Piaget’s Theory of Cognitive Development on page 79)
Infants
-
- 0 to 6 months— Sensorimotor. Best toy is a musical mobile (Best choice) Toy should be large but soft (2nd best choice)

-
- 6 to 9 months— Object permanence. Best toy teach them to Cover/Uncover This is to teach them that the object is still there even if they can’t see it
 Examples are: Jack-in-the-Box and Peek-a-Boo
Examples are: Jack-in-the-Box and Peek-a-Boo
Toy should be large but firm
Worse toy after 6 months is the Musical Mobile because of the risk of strangulation
-
- 9 to 12 months— Vocalization. Best toys are speaking or verbal toys
Good list of toys are: Tickle me Elmo, Woody Cowboy, See and Say- Barnyard Friends, Talking books
For purposeful play, the infant should be at least 9 months or older
- These words mean purposeful play: build, sort, stack, make, and construct
- Baby in womb for 9 months, another 9 months for purposeful play
Toddlers
-
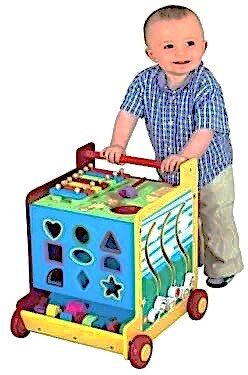 1 to 3 years— Work on Gross Motor skills, which is running, jumping
1 to 3 years— Work on Gross Motor skills, which is running, jumping
Best toys for this age group are Push/Pull toys
Examples are: Lawn mowers, Wagon, dog with floppy feet
They can paint (They use the hand to paint)
They are characterized Parallel Play (think terrible two)
Preschoolers
-
 3 to 6 years— Work on fine motor skills
3 to 6 years— Work on fine motor skills
Therefore, preschoolers have finger dexterity; hence, can write, draw, use colored pencils, scissors
Work on balance—Dance, ice skates, tricycles, tumbling They are characterized by Cooperative Play
- Need to cooperate in Preschool (= Pretend)
- You’d be the sheriff, I’ll be robber …
Highly imaginative
School age
-
- 7 to 11 years— Concrete
Characterized by the “3 Cs”
- Creative—Give them blank paper to draw, they like to get involved … Toys: Legos, Transformers
- Collective—Baseball cards, Webkinz, Barbies, Beanie Babies
- Competitive—Winner/losers
Adolescents
-
- 12 to 18 years— Peer group association

Allow adolescents to be in each other’s rooms unless one of them has been/is
- Recently post-op for <12 hrs
- Immunosuppressed
- Contagious
Note: When given a variety of ages to choose from, always go younger because children regress, when sick you want to give them time to grow
Laminectomy (78:32)
Lamina: the vertebral spinous process (bumpy bones along backbone) Ectomy: removal
Laminectomy is the removal of the vertebral spinous process
Question
Why perform a laminectomy?
-
- To relieve nerve root compression … In other words, cutting away the bony prominence gives the nerve more room
Question
What the S/Sx of nerve root compression?
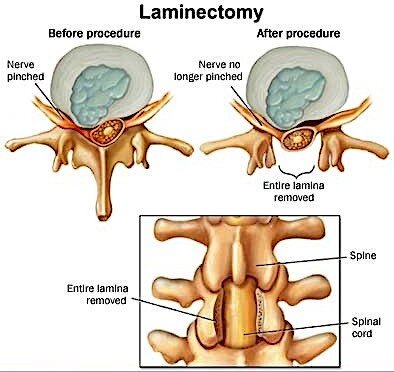
-
- The 3 “Ps”
- Pain
- Paresthesia (tingly)
- Paresis (muscle weakness)
When you get a laminectomy question, pay attention to location, location, location
-
- There are 3 different locations where laminectomy is performed
- Cervical
- Thoracic
- Lumbar
- Cervical—neck
- What is the most important pre-op assessment for cervical?
- Cervical innervates the diaphragm and the arms
- First, assess for breathing
- Next, check functions of arms/hands
- Post-op complication
- Watch for pneumonia
- What is the most important pre-op assessment for cervical?
- Thoracic—upper back
- What is most important pre-op for thoracic?
- Thoracic innervates gut/abdominal muscles … Assess cough and bowels (cannot cough when you cannot contract abs)
- Post-op complication
- Pneumonia and paralytic ileus
- What is most important pre-op for thoracic?
- Lumbar—lower back
- What is most important pre-op for lumbar?
- Lumbar innervates Bladder and legs … Assess for urinary retention or last time pt voided or is the bladder empty
- Next best answer is to evaluate leg functions
- Post-op complication
- What is most important pre-op for lumbar?
o Urinary retention and Leg problems
-
- Lumbar = Legs, Urinary retention
Postop Laminectomy
-
- Number 1 answer for postop laminectomy, including spinal surgery, is log roll
- Better pick log roll
Mobilizing pt after laminectomy or spinal surgery
-
- Do not dangle these pts—have them seat at the edge of the bed
- They should go from supine to walking as soon as possible
- Can they sit on bed long enough to overcome orthostatic hypotension?
- Yes, but not for 10 to 15 minutes
- Do not allow pt to sit for more than 30 minutes
- So, what post-op order would you question for a laminectomy?
- Up in chair for 1 hour TID
- These pts may
- Walk, stand, lie down without restriction
Sitting is bad
Question
You are caring for a pt with a lumbar oligodendrogliocytoma. What is the #1 problem?
- Airway
- Ileus
- Cardiac arrhythmia
- Urinary retention
Answer
Who cares what oligodendrogliocytoma is. The lesion is in the lumbar spine. Therefore, we should assess for urinary retention, then for leg problems
-
- If the question instead mentions lumbar abscess or lumbar surgery, lumbar ependymoma, the answer would be the same
Note
Recap—Laminectomy
- Cervical = Neck and Arms
- Thoracic = Lungs and GI
- Lumbar = Bladder and Legs
Typically there are no chest tubes with Laminectomy. However, the anterior thoracic will have chest tubes
-
- What does anterior thoracic means?
- From the front through the chest to the spine
- What does anterior thoracic means?
Laminectomy with fusion
-
- This involves taking a bone graft from (1) the iliac crest and (2) the spine
- Bone from your hip is taken and put it in place so no bone-to-bone
Questions
Of the two incisions, which site has the most Pain?
-
- THE HIP
Of the 2, which one will have/need the most Bleeding/Drainage?
-
- THE HIP
- This is where the HEMOVAC, JP will be
Of the 2, which one has the higher risk of infection?
-
- They are equal
Of the 2, which one has the higher risk for rejection?
-
- The spine
Since the hip gives more problems, surgeons want to get rid of hip incision. Why?
-
- Because, it is shorter recovery … It cuts the infection in half … It decreases the drainage by 80% … Decreases the pain by 80%
- That is why surgeons are using cadaver bone from banks because the risk of rejection is very low
- Bone are not protein and protein is what triggers the antigen-antibody response
Discharge Teaching?
There are 4 temporary restrictions and 3 permanent
-
- Temporary restrictions … (6 weeks)
- Do not sit for >30 minutes
- Lie flat, log roll for 6 weeks
- Don’t drive for 6 weeks
- Don’t lift more than 5 lbs for 6 weeks (gallon of milk) Permanent restrictions
- Permanent restrictions
- Laminectomy patients will never be allowed to lift by bending at waist (use knees)
- Cervical laminectomy should never be allowed to lift anything over the head
- No horseback riding, off trail biking, jerky amusement park rides, etc. …
Note
This lecture on laminectomy can be used to get any spinal cord question correct … Pay attention to location
Lecture 8 • Mark Klimek • 53:53
You will be asked to prioritize different pts based on lab values
Therefore, it is not good enough to simply know the normal/abnormal lab values You would have to rank or prioritize pts based on abnormally critical lab values
Use the “ABCD” scheme to prioritize pt based on lab values
-
- Low priority
- A is low priority … This lab result can be ignored for a few hours or, if late at night, until very early morning
- B is concerning … This lab result needs to be closely monitored
- High priority
- C is critical … You need to do something for this lab
- Low priority
The RN does the first set of assessments for Levels C or D … Example: V/S, lung and heart auscultations, abdominal exam, etc.
-
-
- D is highest priority … Stay at the bedside
-
Lab Values (05:11)
| Lab | Range | “ABCD” Scheme | |
| Creatinine (Cr) | Best indicator of kidney or | 0.6 to 1.2 | Level A |
| renal function | Level B if dye procedure | ||
| (such as a catheterization) is | |||
| involved | |||
| INR | Monitors coumadin … Also reflects PT (or Prothrombin time) | 2 to 3 | Level C when 4 and above |
Potassium (K+) Blood chemistry
- Action to take in following order … Hold Coumadin Focus Assessment for bleeding
Prepare to give vit K Call HCP
3.5 to 5.3
- LOW potassium … Action to take in the following order … Nothing to hold Assess heart (EKG) Prepare to give K+ Call HCP
- HIGH potassium (bet 5.4 and 5.9) … Action to take in the following order … Hold K+
Assess heart (EKG) Prepare to give Insulin/Kayexelate Call HCP
- HIGH potassium (6 or more) … Action to take in the following order … Hold K+ Assess
heart (EKG) Prepare to give Insulin/Kayexelate STAT Call HCP, stay with pt
Level C if Low Level C if High Level D if over 6
pH Blood chemistry 7.35 to 7.45 Level D if pH in the 6s
Action to take … Nothing to hold Assess V/S Nothing to prepare Call HCP
| BUN Waste product in blood (Blood urea
nitrogen) |
8 to 25 | Level A |
|
||
| Hemoglobin (Hb) Blood | 12 to 18 | Level B if 8 to 11
Level C if <8 |
Prepare blood Call HCP |
||
Bicarbonate 22 to 26 Level A
CO2 Level C if in the 50s
Level D if in the 60s or higher
|
||
| Hematocrit (Hct) Assess for dehydration | 36 to 54 | Level B |
| O2 or PaO2 Blood chemistry | 78 to 100 | Level C if 70 to 77 Level D if in the 60s or lower, respiratory failure |
Treatment: Give the O2 to pt and increase the rate of fluid administration usually solve the problem
|
||
O2 Saturation 93 to 100 Level C if <93
|
||
| BNP B >100 indicates CHF. Monitor (Brain natriuretic pt for sign of CHF
peptide) |
<100 | Level B if >100 |
Sodium (Na) Electrolyte
Level B if abnormal
Level C if abnormal and there is change in pt’s LOC
135 to 145
-
- Action to take for a Level B … Nothing to hold Assess for fluid overload (hypOnatremia) or dehydration (hypERnatremia) Prepare for furosemide (hypOnatremia) or IV fluid (hypERnatremia) Call HCP
- If there is a change in LOC, pt becomes level C and a safety issue
- CD4 >200 but <500 is HIV
- CD4 <200 is AIDS
- Action for WBC, ANC and CD4 … Assess and put on pt neutropenic precautions
o Refer to neutropenic precautions below
| WBC | Total 4,000
to 11,000 |
Level C <4,000 |
| ANC (Absolute neutrophil count) | >500 | Level C <500 |
| CD4 | >200 | Level C <200 |
| Platelet (PLT) | 150,000 to
450,000 |
Level C if <90,000
Level D if <40,000 |
| RBC
(Red blood cell) |
4 to 6 million | Level B if abnormal |
Platelet and RBC (Continued onto Lecture 9)
Neutropenic Precautions
Five Deadly “Ds”
- The following are 5 priority pts based on their lab values
- The NCLEX exam will not put one of the followings against another
- K+ >6
o pH in the 6s
-
- CO2 in the 60s
o pO2 <60
-
- Platelets <40,000
- Strict hand washing
- Vital q4 hrs
- Dedicated stethoscope, BP cuff
- Reverse/protective isolation
- Shower BID with microbial soap
- Avoid crowds
- Private room
- Limit staff/visitors
- No fresh flowers/potted plants
- No raw fruits/veggies/undercooked meat
- No water pitcher standing for over 15 minutes
- Check WBC daily
- No indwelling catheters
- Do not reuse cups or disposable plates
Lecture 9 • Mark Klimek • 56:14
Platelet and RBC (Continued from Lecture 8)
| Lab | Range | “ABCD” Scheme |
| Platelet (PLT) | 150,000 to
450,000 |
Level C if <90,000
Level D if <40,000 |
| RBC
(Red blood cell) |
4 to 6 million | Level B if abnormal |
Neutropenic Precautions
Five Deadly “Ds”
- The following are 5 priority pts based on their lab values
- The NCLEX exam will not put one of the followings against another
- K+ >6
o pH in the 6s
-
- CO2 in the 60s
o pO2 <60
-
- Platelets <40,000
- Strict hand washing
- Vital q4 hrs
- Dedicated stethoscope, BP cuff
- Reverse/protective isolation
- Shower BID with microbial soap
- Avoid crowds
- Private room
- Limit staff/visitors
- No fresh flowers/potted plants
- No raw fruits/veggies/undercooked meat
- No water pitcher standing for over 15 minutes
- Check WBC daily
- No indwelling catheters
- Do not reuse cups or disposable plates
Psychiatric Drugs
ALL psychiatric drugs cause low BP and weight changes—usually weight gain
Major Classes Phenothiazines
-
- First generation or typical antipsychotics
- All end in “ZINE”
- Example: Thorazine, Compazine
- They don’t cure … They just reduce symptoms
- We use ZINEs for the ZANY (Cuckoos) … Antipsychotics
- In small doses, they are antiemetics (to treat vomiting)
Phenothiozines are major tranquilizers
-
- Major tranquilizers—big guns psych meds—are Antipsychotics
Analogy
-
-
- Aminoglysoside are to Antibiotics what Phenothiazines are to Antipsychotics
- Antipsychotics S/Es = “ABCDEFG”
- Anticholinergic (dry mouth, urinary retention)
- Blurred vision
- Constipation
- Drowsiness
- EPS (tremors, Parkinson)
- Foto sensitivity
-
o aGranulocytosis (low WBC count, immunosuppressed)
Teach patient how to recognize and report sore throat and symptoms of infection
Question
-
- What is the nursing action when someone presents with a S/E?
- Educate
- What is the nursing action when someone presents with a S/E?
Question
-
- What is the nursing action when someone presents with a Toxic effect?
- HOLD the drug Notify HCP
- What is the nursing action when someone presents with a Toxic effect?
Note
-
- The #1 nursing diagnosis for “ABCDF” S/Es is to teach pt about SAFETY
- The #1 nursing diagnosis for “G” S/Es is to teach pt to report signs of infections to HCP
Decanoate or “Caprate” form of a medication
-
- The long-acting form of a drug
- Sometimes denoted with the letter “D”
- IM form given for non-compliance
- Often Court-ordered
Tricyclic Antidepressants
-
- Grandfathered into the NSSRI (Non-selective serotonin reuptake inhibitor) group
- Mood elevators (Happy pills)
- Elavil (elevates), Trofranil, Aventyl, Desyrel
- Elevates the mood
- Side effects of TCA are Anticholinergic (especially, dry mouth) Blurred Vision
Constipation Drowsiness Euphoria (happy)
Must take meds for 2 to 4 weeks for beneficial effects
-
- So, after the first week of antidepressant therapy, pt will complain the drug is not working
- Teach pt that the medication takes about 2 to 4 weeks to reach therapeutic effects
Benzodiazepines
Naming of antipsychotics
- If you want to put someone asleep, give him the ZZzzs
- Zines for the Zany (major antipsychotics)
- Zeps for the minor antipsychotics
o If you are old enough, you may answer that question … What do you find at a Zeppelin concert?
Minors on tranquilizers
-
- Anti-anxiety, minor tranquilizers
- Always have ZEP in the name
- Remember ZZzzs for falling/going to sleep
- Many benzodiazepines end in “Pam” or
“Lam”
-
- Prototype: Valium, induction of anesthetic, muscle relaxant, alcohol
- Can be used as
- Seizures medications
- Preop induction of anesthesia
- Muscle relaxants
- EtOH withdrawal medications
- Ventilation—medication to relax and calm down pts on a ventilator
- Benzos work quickly … But do not take them for more than 2 to 4 weeks
Administer major and minor tranquilizers at the same time. Why?
-
- The major antipsychotics take a long time to start working
- The minor antipsychotics start working right away
- Both are administered at the same time
- Example: pt is usually put on Valium and Elavil at the same time
- Valium is discontinued in 2 to 4 weeks once Elavil kicks in
Note
A similar example for giving major and minor tranquilizers together is the concurrent use of Heparin and Coumadin (warfarin)
-
- Heparin works right away but a pt should not be on it for a long time
- Coumadin takes a few days to start working but a pt can be on it for the rest of his life
S/Es of Benzodiazepines are “ABCD”
-
- Anticholinergic
- Blurred Vision
- Constipation
- Drowsiness
Monamine Oxidase (MAO) Inhibitors
-
- Antidepressant
- Depression is thought to be caused by norepinephrine, dopamine, and serotonin in brain
- Name of MAOIs starts with
- MARplan, NARdil, PARnate the beginnings—all rhyme
- S/E of MAOIs
- Anticholinergic
- Blurred Vision
- Constipation
- Drowsiness
Teaching Points
-
- Avoid tyramine-containing food … May cause Hypertensive Crisis
- Food with tyramine
- Fruits/Veggies—Avoid salad “BAR”: Bananas, Avocados (guacamole), Raisins (dried fruit)
- Grains—Ok to have, except Yeast
- Meats—No organs liver, kidney, tripe, heart, no preserved meats (smoked, dried, cured, pickled, hot dogs)
- Dairy—No chees except for mozzarella, cottage cheese (no aged cheese)
- No EtOH, elixirs, tinctures (iodine/betadine) caffeine, chocolate, licorice, soy sauce
Lithium
-
- Used for treating Bipolar disorder—it decreases the mania LI = BI
- S/E: Very Unique—acts more like an electrolyte—think: Potassium/Lithium
- The 3 Ps as S/Es
- Peeing (Polyuria)
- Pooping (diarrhea)
- Paresthesia (earliest sign of electrolyte imbalance)
The earliest sign of electrolyte imbalance is Paresthesias = Numbness and Tingling
Toxic effects of lithium
-
- Tremors
- Metallic taste
- Severe diarrhea
Question
What is the #1 nursing intervention in a pt on lithium presenting with peeing/pooping all the time?
-
- #1 intervention
- Give pt fluids
- The above S/Sx are S/Es—expected
- Monitor sodium
- Low sodium makes lithium toxic
- High makes lithium ineffective
- Sodium needs to be normal
- #1 intervention
Question
What is the #1 nursing intervention in a pt on lithium presenting with metallic taste and severe diarrhea?
-
- #1 intervention
- Give pt fluids
- Notify the HCP—this is a toxic effect
- #1 intervention
Prozac (fluoxetine)
-
- SSRI, mood elevator
- Side effects of Prozac are
- Anticholinergic
- Blurred Vision
- Constipation
- Drowsiness
- Euphoria (happy)
Causes insomnia so give before noon. If bid, give at 6 a.m. and noon
-
- When changing doses, watch for suicidal risk in adolescents
- Must recently change the dose and be an adolescent of young adult
- When changing doses, watch for suicidal risk in adolescents
HALDOL (haloperidol)
-
- Tranquilizers (basically same as Thorazine)
- S/E of Haldol
- Anticholinergic (dry mouth, urinary retention)
- Blurred vision
- Constipation
- Drowsiness
- EPS (tremors, Parkinson)
- Foto sensitivity
o aGranulocytosis (low WBC count, immunosuppressed)
Teach patient how to recognize and report sore throat and symptoms of infection
-
- First generation antipsychotics
- Pts may develop NMS (neuroleptic malignant syndrome) from overdose
- Seen in elderly and young white schizophrenic pts
- High fever over 105
- Their doses should be about ½ usual adult dose
Question
A pt is being treated with an antipsychotic medication. Pt becomes anxious and presents with tremors. What is the nurse intervention to differentiate NMS (neuroleptic malignant syndrome) from EPS (extrapyramidal syndrome)?
-
- Measure the pts’ temperature
- If temperature is WNL, this is EPS
- If temperature is 102 and rising, call the emergency response team and notify HCP … NMS is lifethreatening
- NMS presents with anxiety and tremors, and so does EPS
- Measure the pts’ temperature
Note: With Haltol, there are safety concerns related to the S/Es
Clozaril (clozapine)
-
- Atypical antipsychotic
- Advantage it does not have A-F side effects
- Don’t confuse it with Klonopin/Clonazepam!
- S/Es of clozapine
o aGranulocytosis! It is worse than cancer drugs and can trash the pt’s bone marrow
Note
-
- Geodon (ziprasidone) has a black box warning
- Prolong the QT interval, which can cause sudden cardiac arrest
- Do not use in pts with cardiac condition
Note: Second generation antipsychotics end in “Zapine”
Question
What is the #1 nursing intervention in a pt taking Clozaril (clozapine)
-
- Monitor the WBC
Zoloft (Sertraline)
-
- Antidepressant
- Can cause insomnia
- Interact with the followings because they are not metabolized in the liver
- St. John’s Wort and cause serotonin syndrome
- Warfarin and cause bleeding
- S/E of serotonin syndrome is “SAD Head”
- Sweating
- Apprehensive (impending sense of doom)
- Dizzyness
- Headache
Note: The nurse should anticipate lowering the dose of sertraline (Zolof) of a pt on St. John’s Wort and Warfarin
Lecture 10 • Mark Klimek • 87:50
Maternity and Neonatology
Determining the estimated date of delivery
-
- Use the Naegele rule—take first day of last menstrual period (LMP), add 7 days and subtract 3 months from it
- For instance, if the last menstrual period of a pt was between June 10 and 15
- The estimated date of delivery = March 17
- Use the Naegele rule—take first day of last menstrual period (LMP), add 7 days and subtract 3 months from it
Weight gained during pregnancy
If weight gained during pregnancy is within
+/–1 to 2 lbs of the ideal weight for the gestational week … Pt is WNL
If weight gained is within
+/–3 lbs … Assess her
+/–4 lbs or more… There is trouble
o perform a BPP on the fetus
-
- 1st trimester (12 weeks)
- 1 lb per month = Total of 3 lbs
- 2nd and 3rd trimesters
- Add 1 lb every week
- The ideal weight gained during pregnancy
- 28 lbs, plus or minus 3
- Between 25 to 31 lbs
- 1st trimester (12 weeks)
Alternative method
A quick and dirty way to come up with the ideal weight gained during pregnancy is to
-
- Take the number of weeks gestation minus 9
Question
A woman is in her 28th week gestation. She gained 22 lbs, what is your impression?
-
- Using the long method
- First trimester (12 weeks) … She gained 3 lbs
- 28 weeks minus 12 weeks = 16 weeks
- Therefore, she would add an extra 16 lbs on her weight
- 3 + 16 = 19 lbs … She has 3 lbs extra than her ideal weight
- Therefore, assess the pt
- Alternatively, subtract 9 from the number of weeks gestation
- Using the long method
o 28 – 9 = 19 lbs
Question
A pregnant woman at 31 weeks gestation gained 15 lbs. what is your impression?
-
- Using the short method, this pt ideal weight should be
o 31 – 9 = 22 lbs
-
-
- However, 22 – 15 = 7 lbs less than the ideal
- Therefore, the nurse needs to assess the biophysical profile (BPP) on the fetus
-
Fundal Height
-
- Fundal height cannot be palpated until week 12
- That when the fundus is midway between the umbilicus and the pubic symphysis
- The fundus can be palpated at the umbilicus between 20 and 22 weeks
- Fundal height cannot be palpated until week 12
What is the significance of being able to palpable fundal height?
-
- The examiner should be able to determine in what trimester the pregnancy is
- In case pt is unconscious, for instance
- It has diagnostic significance as well … A much bigger than normal fundus may indicate molar pregnancy
- The examiner should be able to determine in what trimester the pregnancy is
Positive Signs of Pregnancy
The Boards test positive signs and everything else
- Fetal skeleton on x-ray
- Presence of fetus on ultrasound
- Auscultation of fetal heart (Doppler)
- Examiner palpates fetal movement (outline)
- Not the mother but the examiner
Ranges of Values
In OB, there are 3 types of questions regarding range of values
For instance, the fetal HR can be heard first between 8 to 12 weeks gestation Quickening (baby Qicks) may be first felt between 16 to 20 weeks gestation Therefore, if the question ask
When would you first?
-
-
- Fetal Heart: 8 weeks
- Quickening: 16 weeks
- This is the earliest date
-
When would you most likely?
-
-
- Fetal Heart: 10 weeks
- Quickening: 18 weeks
- This is the date midway in the range
-
When should you by?
-
-
- Fetal Heart: 12 weeks
- Quickening: 20 weeks
- This is the latest date
-
Maybe Signs of Pregnancy
- Positive urine/blood hCG tests
- A positive pregnancy test may result from other conditions
- For instance, cancer
- Chadwick sign—cervical color change to cyanosis (Cs)
- Bluish discoloration of the vulva, vagina and cervix
Goodell sign—good and soft
-
- Softening of the cervix
Hegar sign—uterine softening
-
- Softening of lower uterine segment
Chadwich Goodells Hegar
-
- All 3 signs are in alphabetical order and
- Move up from the vulva, vagina, cervix to the uterus
Patient Teaching for Prenatal Visit
During pregnancy, pt is advised to go for prenatal visits as follows
-
- Once a Month until week 28
- Every other week between 28 and 36
- Once a week after week 36 until delivery or week 42, whichever comes first
- At week 42, delivery can be induced or by C-section
Question
If a woman comes in for her 12th week prenatal checkup, when is her next prenatal visit?
-
- Her next visit is at 16 weeks
Lab Values
UWorld
Hemoglobin (Hb)
- 1st & 3rd trimester
- 11 g/dL
- 2nd trimester
- 10.5 g/dL
- If Hb <9, anemia evaluation
Hemoglobin (Hb) level will fall during pregnancy
-
- Normally Hb in female = 12 – 16
- A pregnant woman can tolerate lower levels of Hb
- First Trimester: Hb can fall to 11 and be perfectly normal
- Second Trimester: Hb can fall to 10.5 and be perfectly normal
- Third Trimester: Hb can fall to 10 and be perfectly normal
Question
How do you treat morning sickness?
-
- Morning sickness is usually seen during the 1st trimester
- Treatment: Dry carbohydrates—not before breakfast but—before pt gets out of bed
Question
How do you deal with urinary incontinence?

-
- Urinary incontinence is seen in the 1st and 3rd trimesters
- Pt needs to void every 2 hours from the day she gets pregnant until 6 weeks postpartum
Question
A pregnant pt complains of difficulty breathing. What should you advise her to do?
-
- Difficulty breathing is a problem during the 2nd and 3rd trimesters
- Advise pt to assume to tripod position
- Tripod position is a physical stance often assumed by people experiencing respiratory distress
Figure 7. Tripoding.
-
-
- The pt will be leaning forward with hands on knees or the surface of a desk or table
-
Question
A pregnant pt complains of back pain. What should you advise her to do?
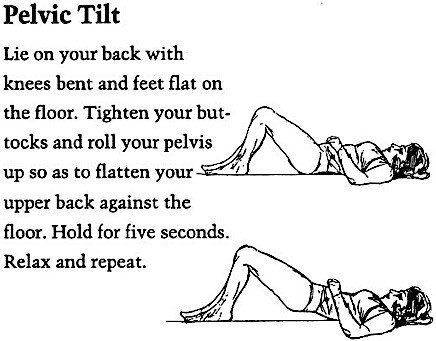
-
- Back Pain is seen during the 2nd and 3rd trimester
- Advise pelvic tilt exercises to pt
Labor and Birth
What is the truest most valid sign that she is in labor?
-
- The truest most valid sign of labor is the
onset of regular/progressive contractions
To Know
-
- Dilation is opening cervix from 0 to 10 cm
- Effacement is thinning of the cervix. It goes from thick to 100% efface (thin like paper)
- Station is the relation between fetal presenting part and the mother’s ischial spines (know this)—the narrowest part of the pelvis
- Positive numbers mean the baby has made it through this tight squeeze—good to go
Positive numbers = Positive news
-
-
- If a baby stays at a –3, –2, –1, it can’t get through vaginally. It needs C-section for delivery
- Engagement is station zero—this means the presenting part is at the ischial spines
-
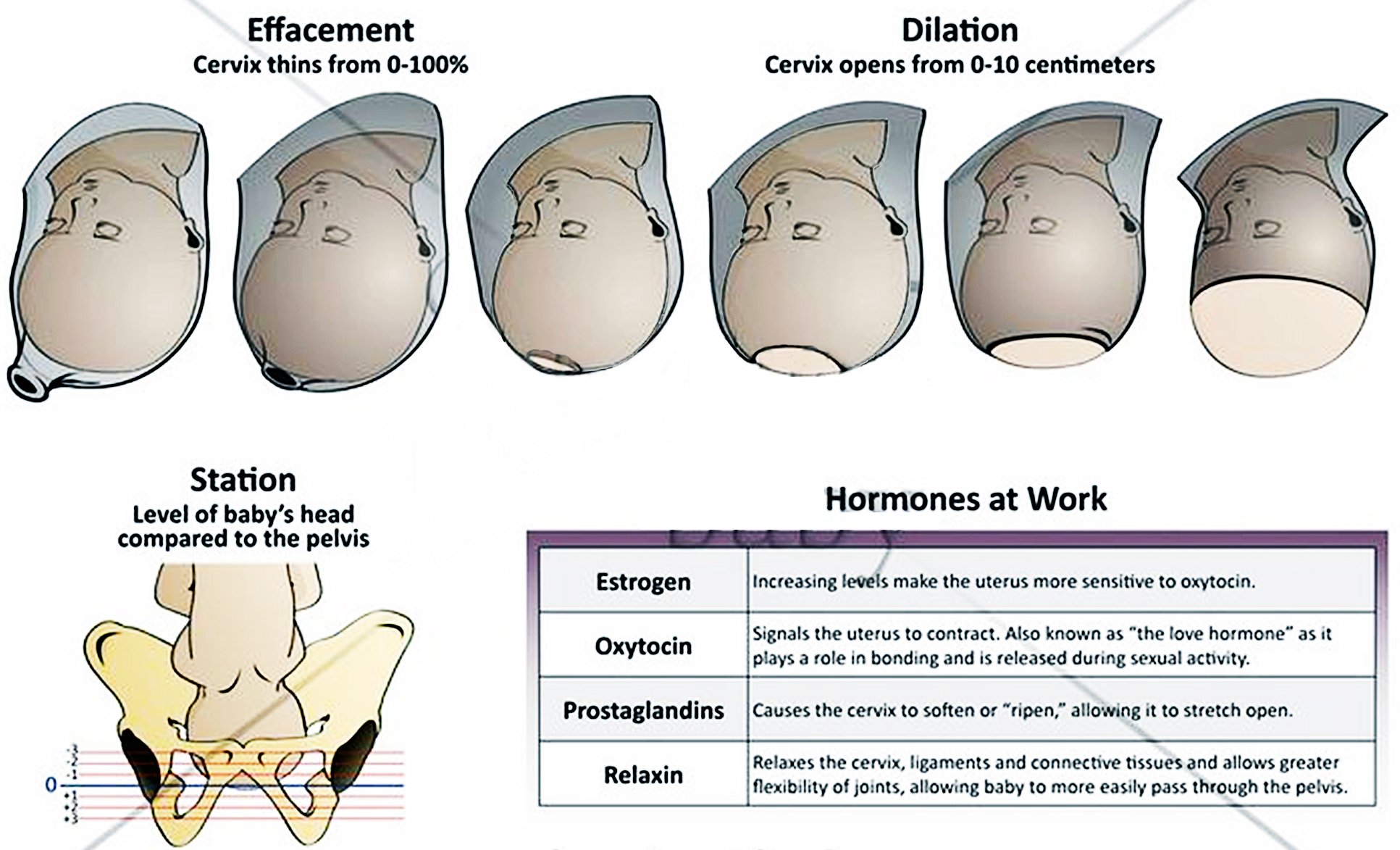
Lie is relationship between the spine of the mother and spine of the baby
-
- You want a vertical lie—compatible with vaginal birth
- If the mother’s spine and the baby’s spine is parallel—we got a baby
- If lie is perpendicular—tranverse lie = Trouble … C-section
- If we got them perpendicular, we’ve got trouble—T
- You want a vertical lie—compatible with vaginal birth
Most common presentation is ROA or LOA—that’s the guess—don’t bother memorizing
-
- ROA (right occiput anterior)
Note
Before giving digitalis, always take an apical HR (heart rate)
-
- LOA (left occiput anterior)
- Pick ROA before LOA
Delivery of the Fetus and the Placenta
-
- There are 4 stages of labor
Stage 1 Onset of Labor—It has 3 phases
-
- Latent—cervical dilation from 0 to 4 cm
- Phase 1
- Contractions are 5 to 30 minutes apart, lasting 15 to 30 seconds
- Mild intensity
- Active—cervical dilation from 5 to 7 cm
- Phase 2
- Contractions are 3 to 5 minutes apart, lasting 30 to 60 seconds
- Moderate intensity
- Transition—cervical dilation from 8 to 10 cm
- Phase 3
- Contractions are 2 to 3 minutes apart, lasting 60 to 90 seconds
- Strong intensity
- Latent—cervical dilation from 0 to 4 cm
Question
A pregnant woman comes in to L&D (labor and delivery). She is 5 cm dilated, with contraction 5 minutes apart, lasting 45 seconds. What phase of labor is the pt in?
-
- The pt is in ACTIVE phase
One good studying strategy to use for memorizing the 3 phases of Stage 1 labor is to know everything about the Active (or Phase 2) of Stage 1
-
- Once you know the upper and lower limit values, you can deduce the values of Phase 1 and Phase 3
- Phase 2 — Contractions: 3 to 5 minutes and last 30 to 60 seconds
- Once you know the upper and lower limit values, you can deduce the values of Phase 1 and Phase 3
Stages and Phases of Labor
-
- Stage 1—Onset of Labor Cervical Dilation and Effacement
- Phase 1—Latent
- Phase 2—Active
- Phase 3—Transition
- Stage 2—Delivery of Baby
- Stage 3—Delivery of Placenta
- Stage 4—Recovery: 2 hours until bleeding stops
- Stage 1—Onset of Labor Cervical Dilation and Effacement
HESI Questions
What is purpose of uterine contraction in first stage?
-
- Dilation and effacement of the cervix What is the purpose in 2nd stage?
- Delivery of baby
What is the purpose 3rd stage?
-
- Delivery of placenta
What is the purpose of 4th stage?
-
- Stop bleeding
When does postpartum technically begin?
-
- 2 hours after delivery of placenta
Pay attention to whether the question is asking about stages or phases
-
- There are 4 stages
- There are 3 phases, which are part of Stage 1
Questions
What is the #1 priority of second phase?
-
- Pain management
What is the #1 priority of second stage?
-
- Clearing baby’s airway
Questions
What is the #1 priority of third phase?
-
- Checking cervical dilation, Helping pregnant mother with breathing and pain management What is the #1 priority of third stage?
- Assess the placenta for smoothness and intactness, and for 3-vessel (not 2) umbilical cord present
Stages and Phases of Labor
-
- Stage 1—Onset of Labor
- Phase 1—Latent … Dilation from 0 to 4 cm
- Stage 1—Onset of Labor
Contractions are 5 to 30 minutes apart, lasting 15 to 30 seconds
Mild intensity
-
-
- Phase 2—Active … dilation from 5 to 7 cm
-
Contractions are 3 to 5 minutes apart, lasting 30 to 60 seconds
Moderate intensity
-
-
- Phase 3—Transition … dilation from 8 to 10 cm
-
Contractions are 2 to 3 minutes apart, lasting 60 to 90 seconds
Strong intensity
-
- Stage 2—Delivery of Baby
- Stage 3—Delivery of Placenta
- Stage 4—Recovery: 2 hours until bleeding stops
Memorize for the following 3 quetions
Uterine contraction should be no longer than 90 seconds and no closer than 2 minutes
Questions
What is a sign of uterine tetany?
-
- No longer than 90 seconds and no closer than 2 minutes
What parameters regarding uterine contraction would make you stop Pitocin?
-
- No longer than 90 seconds and no closer than 2 minutes
What is uterine hyperstimulation?
-
- No longer than 90 seconds and no closer than 2 minutes
Know that phrase
-
- No longer than 90 seconds and no closer than 2 minutes
Assessment of frequency of contraction
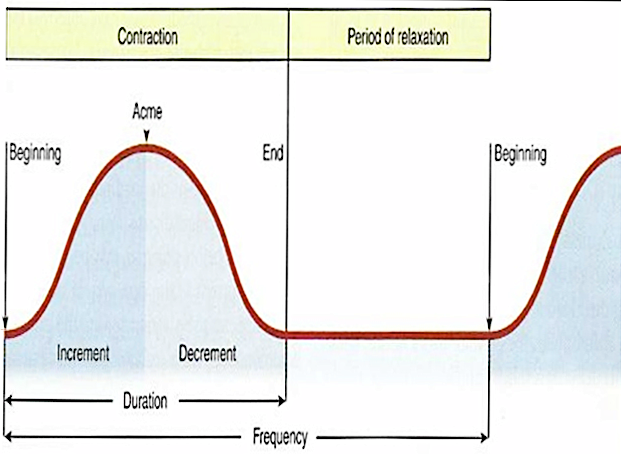
-
- Frequency is from the beginning of one contraction and beginning of the next
Assessment of duration of contraction
-
- Duration of contraction is from the beginning to end of one contraction
Intensity of labor
-
- Assessment of intensity of labor is purely subjective
Teach her how to palpate with one hand over the fundus with the pads of the fingers
Complications of labor
-
- There are 18 complications
- Know them all
- But only 3 protocols—focus on the 3 protocols
Painful Back pain—“OP” = Oh Pain. What do you do?
“OP” … Anything (right or left) occiput posterior
-
- Position—Push
- What position?
- KNEE-CHEST position then
- PUSH with fist into sacrum to use counter pressure
Prolapsed Cord
-
- Push head in off cord and position knee-chest or Trendelenburg
- Prep for C-section
- Think PUSH/POSTION
- Push head off the cord of fetus and position mother to knee-chest
Interventions for all other complications
-
- Tetany
- Maternal hypertension
- Vena cava syndrome
- Toxemia
- Uterine rupture
- All treated the same—with “LION”
- Left side (place mother on the left side)
- IV
- Oxygen
- Notify HCP
- Stop Pitocin (pit) if it was running—the first thing to do
Implement before “LION”

Figure 8. Knee-chest position.
-
- In an OB crisis, if pitocin is running, stop it first. Then, implement “LION”
When to administer systemic pain medication
-
- Do not administer a systemic pain medication to a woman in labor if the baby is likely to be born when the med is at its peak … For example
Questions
-
- You have a primagravida at 5-cm dilated who wants her IV push pain med. What is the nursing intervention?
- Hold the pain medication
- This is because the pt is primagravida and will deliver in about 15 to 30 minutes when the medication peaks
- You have a multigravida at 8-cm wants her IM pain med. What is the nursing intervention?
- Do not administer the pain medication Labor and Delivery (Continued onto next lecture)
- You have a primagravida at 5-cm dilated who wants her IV push pain med. What is the nursing intervention?
Lecture 11 • Mark Klimek • 78:29
Labor and Delivery (Continued from previous lecture)
Fetal Monitoring Patterns
There are 7 fetal monitoring patterns to learn … The ones that start with the letter “L” are bad heart tracings. Use the mnemonic “LION” as the nursing intervention
Normal fetal heart rate = 120 to 160 beats per minutes
Low Fetal HR (heart rate)—HR <110
-
- This is BAD
- You do “LION”
- Left side (place mother on the left side)
- IV
- Oxygen
- Notify HCP
- Stop Pitocin (pit) if it was running
- Implement before “LION”
High Fetal HR—HR >160
-
- Document acceleration of fetal HR
- Take the mother’s temp
- Not a high priority … Baby is WNL
Low Baseline Variability
-
- This is BAD
- Fetal HR stays the same—it doesn’t change
- You do “LION”
- Left side
- IV
- Oxygen
- Notify HCP
- Stop pit if it is running (first)
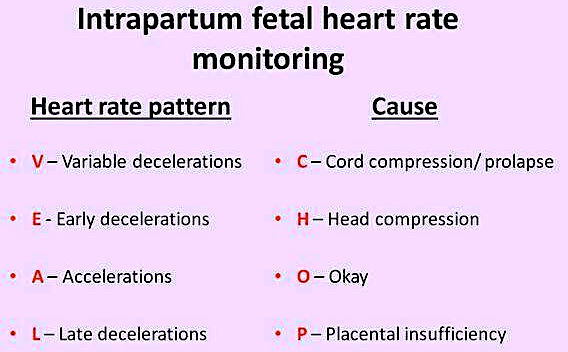
Figure 9. Remember “VEAL CHOP” for the causes of 4 HR patterns.
High Baseline Variability
-
- Fetal heart rate is always changing—This is GOOD
- Document finding
Note
In utero, low variability of V/S is a bad sign but highly variable V/S is a good sign
Early Deceleration
-
- This is normal … No big deal
- Document finding
Variable (VERY) Decelerations
-
- This is very BAD
- This indicates prolapsed cord
- What is the nursing intervention?
- PUSH and POSITION
Late Decelerations
-
- This is BAD
- You do “LION”
- Left side
- IV
- Oxygen
- Notify HCP
- Stop pit if it is running
Recap
-
 Look at the first letter of a fetal heart rate tracing, it is a bad heart tracing if it starts with an “L”
Look at the first letter of a fetal heart rate tracing, it is a bad heart tracing if it starts with an “L”
- Therefore, do “LION” which also starts with the letter “L”
- Variable deceleration is very bad
- PUSH and POSITION)
- Ace of spades means that this answer works every time
- Check the FHR
Second stage of L&D (labor and delivery)
-
- Delivery of the fetus … This is about order.
- Deliver head … The mother needs to stop pushing
- Suction the mouth then the nose … ABC order
- Check for nuchal (around the neck) cord
- Deliver the shoulders, next, the body
- Make sure baby has ID band on before it leaves the delivery area
Third stage of L&D
-
- Delivery of the placenta
- What do you check for with the delivery of the placenta?
- Make sure the placenta is complete and intact
- Check for 3-vessel cord—2 arteries and 1 vein, AVA
Fourth Stage of L&D
-
- Recovery
- There are 4 things you do in the 4th stage, 4 times an hour (every 15 minutes)
- Vital signs: Assessing for shock … Blood pressure goes down, HR goes up … Pt looks pale, cold, and clammy
- Fundus: If it is boggy, massage it … If displaced, catheterize it
- Check perineal pads … If there is excessive bleeding, the pad will saturate in 15 minutes or less
- Roll pt over and check for bleeding underneath her
Recap
-
- 4 things to do every 15 minutes in the 4th stage of labor
- V/S Fundus Peri pads Roll
- 4 things to do every 15 minutes in the 4th stage of labor
Post partum Assessment
-
- Assess every 4 to 8 hours
- Assess for “BUBBLE HEAD”
- Make sure you focus on the 3 designated steps stated as important from BUBBLE HEAD
“BUBBLE HEAD” stands for
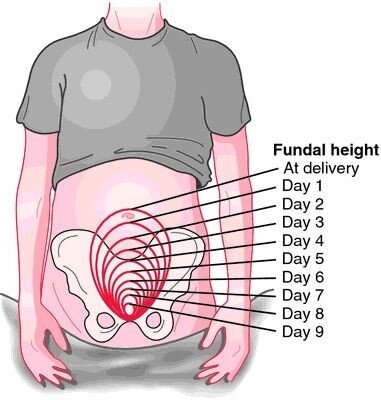
-
- Breasts
- Uterine fundus should be firm … Important
- Massage if fundus is boggy and midline
- Catheterize pt if fundus is boggy and not midline
Question
What should the postpartum uterine tone, height, and location normally be?
-
- The tone of the fundus should be firm, not boggy
- The height of the fundus after delivery should be at the umbilicus (or navel)
- Fundus involutes about 2 cm every day PP (postpartum)
- The location of the uterus should be midline
- If not midline, the bladder is distended
- Bladder
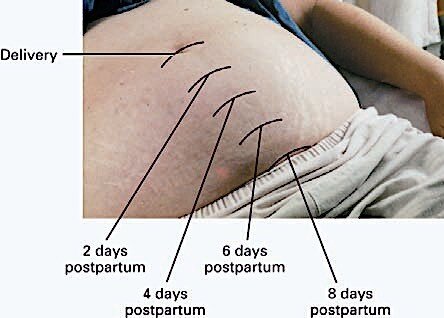
-
- Bowel
- Lochia is vaginal drainage postpartum (Know the order) … Important
- Rubra—red
- Serosa (if your cheeks are rosy)—pink
- Alba (albino)—white
- Moderate amount: 4 to 6 inches on pad in an hour
- Excessive: saturate a pad in 15 minutes
- Episiotomy
- Hemoglobin/hematocrit
Figure 10. Fundal height postpartum.
-
- Extremities—Looking for thrombophlebitis … Important
- What is the best way to determine if a pt has thrombophlebitis?
- Extremities—Looking for thrombophlebitis … Important
The best way is to measure Bilateral calf circumference (Best answer)
Homan sign is not the best answer
-
- Affect—emotional
- Discomforts
Recap
The 3 big things about postpartum on the exam are
-
- Fundus
- Lochia
- Thrombophlebitis
Variations in the newborn
All of the following skin conditions are normal
-
- Milia—White, pinhead-size, distended sebaceous glands on the nose, cheek, chin, and occasionally on the trunk. Usually disappear after a few week of bathing
- Epstein pearls—Palatal cysts of the newborn, which are small white or yellow cystic vesicles
- Mongolian spot—Bluish discoloration in the sacral region of newborn usually seen in African Americans … Carefully document its presence as such action may prevent child abuse charges against parents or caregiver
- Erythema toxicum neoratorum—Described as flee-bitten lesion … pink rash with firm, yellow-white papules or pustule on the face, chest, abdomen, back and buttocks of some newborns. Usually appears 24 to 48 hours after birth and disappear in a few days
- Hemangioma—An abnormal accumulation of blood vessels in the skin of the newborn. It is one of the most common birthmarks associated with childhood and affect 10% of all children
Milia Epstein pearls Mongolian spot Erythema
toxicum neonatorum





Hemangioma
Cephalohematoma vs. Caput succedaneum … Make sure you know these 2
-
- Cephalohematoma—A collection of blood between the periosteum of a skull bone and the bone itself
- Occurs in one or both sides of the head
- Occasionally forms over the occipital bone
- Develops within the first 24 to 48 hours after birth
- Caput succedaneum—An edema of the scalp of the neonate during birth from mechanical trauma of the initial portion of scalp pushing through a narrowed cervix
- The edema crosses the suture lines
- May involve wide areas of the head or it may just be a size of a large egg
- Caput Succedaneum (CS)—Crosses Suture line, and Caput Symmetrical Cephalohematoma Caput succedaneum
- Cephalohematoma—A collection of blood between the periosteum of a skull bone and the bone itself
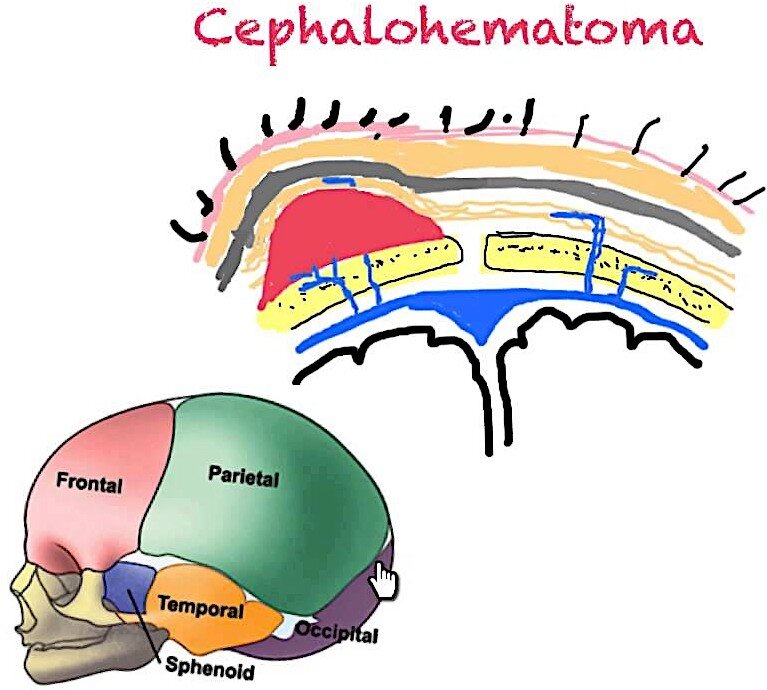
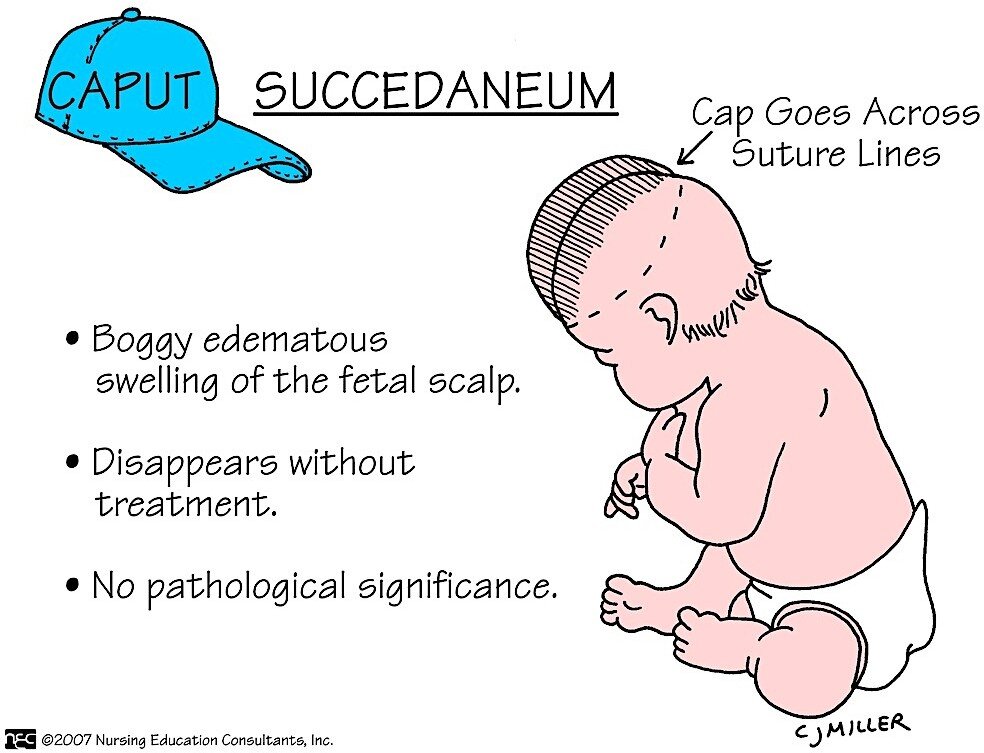
Caput Succedaneum (CS)—Crosses Suture line, and Caput Symmetrical
Hyperbilirubinemia in the Newborn
-
- Physiologic jaundice is normal and appears after 24 hours after birth … Disappears in about one week
- Pathologic jaundice is seen in the 1st 24 hours after birth
Vernix caseosa
Fatty, whitish secretion of the fetal sebaceous gland to protect the skin from amniotic fluid exposure
Acrocyanosis
Blue discoloration of the hands and feet in the newborns during the first few days after birth
-
- Normal finding
and not indicative of poor oxygenation, respiratory distress, or cold stress


Nevi (Telangiectatic nevi)
Nevi or telangiectatic nevi, a.k.a. “stork bites,” are pink and easily blanched skin lesion that appear on upper eyelid, nose, upper lip, lower occipital area, and nape of the neck
-
- No clinical significance
- Disappears by 2 years of age
Port wine stain
Port-wine stain or nevus flammeus is seen at birth and is composed of a plexus of newly formed capillaries in the papillary layer of the corium
-
- Commonly found on the face and neck
- Red to purple, varies in size, shape and location
- Does not blanch on pressure
OB Medications—6
-
- Terbutaline (Brethine)
- Mag sulfate
- Pitocin
- Methergine
- Bexamethasone
- Surfactant
Tocolytics (Stop contractions, stop labor)
-
- Tocolytics are given to women in premature labor that must be stopped
- Terbutaline (Brethine)
- S/E: maternal tachycardia (don’t give with cardiac disease)
- Mag sulfate
- Treatment with Mag sulfate will induce hypermagnesemia, which will cause everything to go down
- HR will go down, BP go down, Reflexes go down, RR go down, LOC go down
Question
So, what is the nursing intervention for hypermagnesemia due to mag sulfate treatment?
-
- Monitor respiration
- If RR <12, decrease dose of Mag sulfate
- Assess for reflexes
- Normal reflex is 2+
- If reflexes are 0 or 1+ … Decrease dose of mag sulfate
- If reflexes are 3+ or 4+ … Increase dose of mag sulfate
- Monitor respiration
Oxytocics (Stimulate and strengthen labor)
-
- Pitocin (Oxytocin)
- S/Es: Uterine hyperstimulation (defined as longer than 90 seconds, closer than 2 minutes) The nursing intervention is to lower the dose of pitocin in case of uterine hyperstimulation
- Methergine
- Causes HTN—if it contracts blood vessels it makes sense that this increases BP
- Pitocin (Oxytocin)
Fetal/Neonatal Lung Meds
-
- Betamethasone (steroid)
- Given to mother IM
- Can repeat as long baby is in utero
- S/E: increase glucose (steroid)
- Surfactant (Survanta)
- Given to baby via transtracheal route
- Given After birth
- Betamethasone (steroid)
Medication Helps and Hints
- What is Humalin 70/30?
Mix of insulin N and R … 70% = N … 30% = R
-
-
- So, if 100 units of 70/30 is given to a pt … the pt gets 70 units of N and 30 units of R
- Or, for 50 units—35 units of N and 15 units of R
- To remember the bigger number, think of a fraction … The numerator N is on top; therefore, Insulin N is the bigger number
-
Question
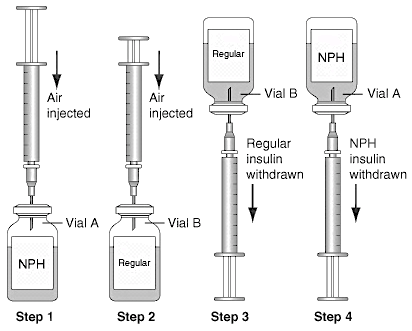
Can you mix insulin in same syringe and how?
-
- Yes, insulin can be mixed in the same syringe
- How do you mix insulin?
- (1) Pressurize vial and (2) Draw up insulin
- To pressurize the vial … Inject air into N, the into R, Draw up R
- To draw up insulin … Think of RN
Needle for Insulin Injections
-
- Know what needle to use for insulin injection?
- Giving an IM injection
- Pick answer in which both answers have a “1” in them
- “I” in IM looks like the “#1”
- Use a 21-gauge, 1-inch long needle
- Giving a SubQ injection
- 5 looks like an “S” in “SubQ”
- Pick the answer that has “5s” in it
- Use a 25-gauge, 0.5 inch needle
Heparin
-
- Given IV or SubQ
- Works immediately
Figure 11. Pressurizing vials with air and drawing up insulin.
-
- Cannot be given for more than 3 weeks (21 days)
After 21 days the body start making antibodies against heparin. Therefore, it is not given for more than 21 days
o Except for Lovenox (enoxaparin)
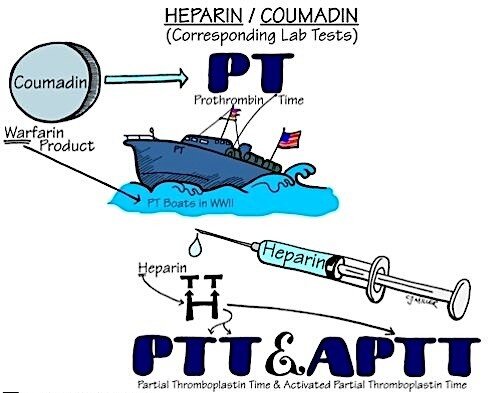
-
- Antidote: Protamine sulfate
- Labs: PTT
- Can be used during pregnancy— Class C medication
Coumadin
-
- Given only PO
- Takes few days to a week to work (likely 4 to 5 days)
- Pts can be on Coumadin for their entire life
- Antidote: Vitamin K
- Labs: PT/INR
- Can’t be used during pregnancy— Class X medication
Note: The only antipsychotic that can be given to pregnant women is Haldol
Diuretics
-
- K-wasting and K-sparing diuretics
- Any diuretic ending in “X,” “Xes” out K
- So, it wastes “K” like Lasix
- PLUS Diuril
- If it does not end in “X,” it is a sparer
- Examples
Brand Generic
-
-
- Aldactone Spinorolactone
- Adactazide Spinorolacone-Hydrochlorothiazide
- Modurectic Amiloride-Hydrochlorothiazide
- Lasix Furosemide
- Bumex Bumetanide
- Clotrix Clotrimazole
- Esidrex Hydrochlorothiazide
- Demadex Torsemide
- Diuril Chlorothiazide
-
Baclofen and Cyclobenzaprine
-
- 2 muscle relaxants to know for the NCLEX
Brand Generic
-
-
- Lioresal Baclofen
- Flexeril Cyclobenzaprine
- The 2 things being tested on the board are
- The 2 S/Es
-
- Fatigue/Drowsiness
- Muscle weakness (paresis)
-
- The 3 things to teach
-
- Don’t drink
- Don’t drive
- Don’t operate heavy machinery
Note: The following phrase help you remember baclofen as a muscle relaxant … “When you are on baclofen, you are on your back loafing”
Pediatric Teaching
Piaget’s Theory of Cognitive Development—4 Stages

-
- There is some overlap with Piaget’s Theory of Cognitive Development and toy appropriateness based on age on page 50
- Make sure not to confused between the two
Sensorimotor—0 to 2 years
-
- They only think about what they are sensing right now
- You can teach only in the present (while you are doing it)
Think Present Tense
-
-
- Just tell them
- Children at this age don’t understand play
- Tell them as it is happening
-
Question
A 19-month-old infant is about to have a lumbar puncture (LP) for csf analysis and culture. How would the nurse teach the child?
-
- Tell the child how the LP is done while it is being done.
- There is no such thing as preop teaching for this age group
- Preop teaching are only for the parents—mom and dad—or guardian
Preoperational (Preschooler)—3 to 6 years
-
- They are fantasy-oriented, imaginative, and illogical, there thinking obeys no rules
- However, they understand the future and they understand the past
Question
A 3-year-old child is schedule for a lumbar puncture (LP) for csf analysis and culture. What is the nurse’s best action to teach the child about the procedure?
-
- Teach 2 hours before …, the morning of …, or the day of the procedure how it will be performed
- They are in the “imaginative” stage … Don’t give them a whole lot of time to imagine the worst
- Teach them what will be done … Future Tense
- They can learn by playing
Concrete Operations—7 to 11 years
-
- “7/11 Grocery Stores are surrounded by concrete”—no trees, no flowers
- Children in this age group are rule-oriented
Live and Die by the Rules and Cannot Abstract
-
-
- There is one way to do things … Everything else is wrong
- Teach them a day or two ahead of time
- Teach them what you’re going to do and how to do skills
- Use age-appropriate reading and demonstration (skill)
-
Question
An 8-year-old child is schedule for a lumbar puncture (LP) for csf analysis and culture. What is the nurse’s best action to teach the child about the procedure?
-
- Use age-appropriate demonstration 1 or 2 days before the procedure
Formal Operations—12 to 15 years
-
- They can abstract and think Cause and Effect
As soon as children become twelve, teach them like an adult
-
-
- This is now a regular Med-Surge question
- When is the first age a child can manage his care?
- 12 years old
- Manage means making decisions which require the person to abstract
-
Question
Which of the following 4 children will be able to manage his own care?
- A 7-year-old with Cystic Fibrosis
- An 8-year-old with Diabetes Mellitus
- A 10-year-old with a scraped knee
- A 13-year-old with Chronic Renal Failure
Answer: (d)
-
- A 10-year-old with a scraped knee as one of the answer choices is a diversion to fool the exam taker. Answer to these questions is not about the severity of the condition but about the age- appropriateness to make decision
- The 10-year-old will Wash, Dry, apply Neosporin and Bandaid the wound as thought … He will continue to do the same thing if the wound becomes is exudating pus and swollen the 4th day … A 12-year-old will likely stop and seek help
- A 13-year-old with chronic renal failure will get help if they are thought to auscultate for a bruit over a shunt and heard nothing on day 3
- This is managing
- This means that knowing what you can do when you can, and seek help when you cannot
- A 10-year-old with a scraped knee as one of the answer choices is a diversion to fool the exam taker. Answer to these questions is not about the severity of the condition but about the age- appropriateness to make decision
Note: Manage = 13-year-lod … Skill = 8-year-old
Seven Principles to Obey When Taking Psychiatric Tests
- Make sure you know what phase of the nurse-patient relationship you are in
- Don’t give/accept gifts in psych
- If a schizophrenic pt gives you flowers, to you the HCP it may be flowers; to him, it may be a marriage proposal
- Don’t give advice!
- If the pt says, “What do you think I should do?” Reply by asking them the same question” “What do you think you should do?”
- The pt won’t be able to blame you in the future even if things work in his favor
- Avoid giving advise in psych
- Never give guarantees
- For instance, “If you cry, you will feel better.”
- There are chances that crying may not help the pt
- Immediacy
- If you are between 2 answer choices and you don’t know which one to pick, pick the one
that keep him talking
-
- Don’t refer to someone
- Concreteness
- Psych pts take you literally. Therefore …
- Never use slang
- If a pt says “I feel rotten.” Don’t reply by saying, “You feel rotten?”
- Don’t ever say to an upset pt to “Chill out!”
- Don’t use figurative speech such as: “What goes around, comes around”
- Empathy
- Empathy is about the nurse accepting the patient’s feelings
- Don’t ever pick an answer that says, “Don’t you worry …” … “You shouldn’t feel …” … “Anybody would feel …” … “I know how you feel …” …
4 steps to answering empathy questions
- Empathy questions will always have a quote
- Role play the feelings (Put yourself in their place) and say the words as you really meant them
- Ask yourself if I said these words, how would I be feeling right now?
- Choose the answer that reflects the pt’s feeling, and ignore what the pt said
Lecture 12 • Mark Klimek • 124:17
Prioritization, Delegation and Staff Management
- This is the most important lecture in the whole review
- There will be at least 15 questions on this section alone
- Most exam takers dead guess in the section
- Learn the material and do not guess
Prioritization
Prioritize—you are deciding which pt is sickest or healthiest… Make sure you know what you’re looking for
Question
For instance, if the question states that there was a disaster in town and you are making room for the wounded, who would you discharge?
- In that case, would you be looking for the highest or lowest priority pt?
- Answer: the lowest priority pt
Question
However, if the question states that you receive handoff end-of-shift reports on 4 pts. Which pt will you check first?
- Answer: the highest priority pt
Answers will usually have 4 parts
- (1) Age, (2) Gender, (3) Dx, and (4) a modifying phrase
- For example: A 10-year-old male with hypospadias is throwing up bile stained emesis
- Age: 10-year-old
- Gender: male
- Diagnosis (Dx): hypospadias
- Modifying phrase: throwing up bile stained emesis
- 2 of which are irrelevant for answering the question
- Age and gender are not important in prioritization
- Age is important in pediatrics
- Of all 4 parts, the modifying phrase is more important
Remember
The modifying phrase is always the most important
Example
Two pts: one has angina pectoris and the other myocardial infarction. Who has the higher
priority pt?
- Answer: The MI pt
- Go by the patient’s condition since there is no modifying phrase
Example
Now modifying phrases are added to each of the diagnosis, which pt becomes the higher priority?
- Pt with unstable BP and Angina
- Pt with stable vital sigh and MI
- Answer: Pt with angina and unstable BP becomes the priority pt
4 rules for prioritization
- Acute beats Chronic
- Meaning that an Acutely ill pt has higher priority than Chronically ill pts
- For instance, among the following pts, a pt with COPD, CHF, or appendicitis, which one has the highest priority?
- Pt with appendicitis (acute condition). Both COPD and CHF are chronic conditions
Fresh Post-op (12 hours) beats medical or other surgical
-
- For instance, among the following pts, a pt 2-hour postcholecystectomy, a pt with COPD, and a pt with acute appendicitis, which pt has the highest priority?
- The 2-hour postcholecystectomy is the highest priority pt … (Fresh post-op, <12 hours)
- Pt with “radical neck dissection” is added to the above scenario?
- The 2-hour postcholecystectomy is the highest priority pt
- Pt with “bilateral above the knee amputation” is added to the above scenario?
- The 2-hour postcholecystectomy is the highest priority pt
- Pt with “right frontal craniotomy” is added to the above scenario?
- The 2-hour postcholecystectomy is the highest priority pt
- For instance, among the following pts, a pt 2-hour postcholecystectomy, a pt with COPD, and a pt with acute appendicitis, which pt has the highest priority?
The point here is that surgery less than 12 hours takes precedence over medical and other surgical conditions
- Unstable beats Stable
- This means that an Unstable pt has a higher priority over Stable pts
How to determine that a pt is stable or unstable?
Word description that makes a pt stable Word description that makes a pt unstable
-
- Stable Unstable
- Chronic illness Acute illness
- Post-op greater than 12 hours Post-op less than 12 hours
- Local or regional anesthesia General anesthesia in the first 12 hours
- Lab abnormalities in the A or B level
- Creatinine, BUN, Hemoglobin 8 to 11, Bicarb, elevated Hematocrit, elevated BNP, elevated Na level, RBCs off
- Lab abnormalities in the C or D level
- INR in the 4s, K in the 6s, pH in 6s, CO2 in the 50s, low O2 sat, high WBC, low ANC, low CD4, low Platelets
Word description that makes a pt stable Word description that makes a pt unstable
-
- Ready for discharge, To be discharged, Admitted longer than 24 hours
- Newly diagnosed, Newly admitted, Not ready for discharge, Admitted less than 24 hours
- Unchanged assessment Changing or changed assessment
- Experiencing the typical expected S/Sx of the disease with which they were diagnosed
- Experiencing unexpected S/Sx
Example
Which of the following pt is the highest priority?
- A 16-year-old female with meningococcal meningitis who has had a temp of 103.8 ºF since she was admitted 3 days ago
- 67-year-old male with IBS (irritable bowel syndrome) who spiked a temp of 103.4 ºF this afternoon
Answer: the 67-year-old pt has the highest priority
-
- 16-year-old: Dx: meningococcal (acute)—high
- Who has had (constant)—low
- Temp of 103.8 (expected)—low
- Admitted 3 days ago (>24 hours)—low
- 67-year-old: Dx: Irritable bowel syndrome (chronic)—low
- Temp spiked (changed)—high
- This afternoon (acute)—high
- 16-year-old: Dx: meningococcal (acute)—high
Four things that always make you unstable, even if they are expected
-
- Hemorrhage—(but not bleeding)
- High fevers over 105 ºF—can lead to seizure
- Hypoglycemia—can lead to brain damage
- Pulseless or Breathless
- Example, V-fib or asystole
- Exception: At the scene of an unwitnessed accident pulseless and breathless pts are low priority because they are likely dead. Therefore, low priority
 In a mass casualty incident, these 3 things result in a BLACK TAG
In a mass casualty incident, these 3 things result in a BLACK TAG
- Pulseless
- Breathless
- Fixed and dilated pupils (even they are still breathing)
- Therefore, “Tag them black and ship them last”
Tie Breaker Rule
-
- If the above 3 rules result in a tie breaker, use the following as a guide
- The more vital the organ, the higher the priority
- Use this rule with the organ of the modifying phrase and not the diagnosis
- Brain
- Lung
- Heart
- Liver
- Kidney
- Pancreas
Example
- You have a 23-year-old male with CHF (chronic—low) with K (6.6—high), and no EKG changes (constant—low)
- Organ: Heart (potassium)
- Chronic Renal failure (chronic low) with a creatinine of 24.7 (expected—low), and pink, frothy sputum (unexpected—high)
- Organ: Lung (frothy)
- Acute Hepatitis (acute—high) with jaundice (expected—low), increased ammonia (expected—low) who you cannot arouse (unexpected—high)
- Organ: Brain (He Wins!)
Example
Determine whether the following are stable or unstable
-
- Angina pectoris—stable
- Angina pectoris with crushing sternal pain—stable, (expected)
- Angina pectoris not relieved by rest—not stable
Delegation of Responsibility
Do not delegate the following responsibilities to an LPN. An LPN is not allowed to assume the following responsibilities … The LPN
- Cannot start an IV
- Cannot hang or mix IV meds
- Cannot push IV Push meds
LPN can only maintain an IV and document the flow
- Cannot administer blood or deal with Central lines … Including flush, change dressings
- Cannot make the care plan … They can however implement the care plan
- Cannot perform or develop teaching … They can reinforce teaching
- Cannot take care of unstable pts
- Cannot perform the “first” of anything … The first of anything is either making the care plan or assessment
For instance, the LPN
-
- Can perform tube feeding only after the nurse did the first tube feeding
- Can change post-op dressing only after the nurse change the first dressing
- Should they change the first post-op dressing the day of surgery? No
- Can feed stroke pt only after the nurse did the first feeding
- Can ambulate post-op pt only after the nurse had first done so
- Can take pt out of bed post-op only after the nurse had first done so
- Can take a set of V/S post-op only after the nurse had first done so
- Is not allowed to assess: admission, d/c, transfer, or first assessment after a change.
Example
-
- I think I heard new crackles on that guy in Room 52. Who should go assess this pt? … The RN or the LPN?
- The RN must assess the pt since this is a new onset or change of a symptoms
- I think I heard new crackles on that guy in Room 52. Who should go assess this pt? … The RN or the LPN?
Example
-
- So who sould the RN check? And who should the LPN check?
- Angina with crushing substernal chest pain, 3 days ago, on nitro
- Subtotal thyroidectomy done 2 days ago and now states “why are they watching elephants?”
-
- The RN should check the pt with subtotal thyroidectomy (onset of a new and worsening symptom, which may be thyroid storm)
- The LPN should check pt with angina with crushing chest pain (expected)
-
Do not delegate the following responsibilities to a UAP
- Charting—UAP can chart what they did but they cannot chart about the pt. For example,
- They can chart, “side rail is up, bed is lowered, etc.”
- They cannot chart, “patient less anxious, tolerated ambulating well”
- Medication administration—They cannot administer medications unless medication is
- Topical medications, over the counter (OTC) medications, and barrier creams
- Cannot give Nitroglycerin or Neosporin ointments because nitroglycerin and Neosporin are not OTC
- Can they give hydrocortisone cream? No
- Can they give A&D ointment? Yes
- Assessments—Except vitals or Accu-Chek for diabetes
- Treatments—Except for enemas
The RN may delegate ADL (activity of daily living) tasks to a UAP … However, the UAP should never do any ADL task first
What to and not to delegate to the family members and friends of pts
-
- Never delegate to the family safety responsibilities. For example, if a family member or friend of pt tells the RN
- “Would you leave the restraints on my dad off and I’ll call you before I leave?”
- Never delegate to the family safety responsibilities. For example, if a family member or friend of pt tells the RN
The answer is: Do NOT delegate safety responsibility to family members or friends of pts
-
-
- RN cannot delegate safety to a non-hospital caregiver unless the person is trained (seater) on how to do the tasks. The RN must document in the pt’s record what exactly was taught
- Can the mother give insulin shot to her 3-year-old child? Yes, if you teach her and document teaching
- What if a new mother asks the RN to “leave the railing of my baby’s crib down and I will put it back up after finish bathing my baby. You can go about what your business”
-
The RN’s answer should be something similar to that. “Don’t worry about me leaving, I
will stay with you to make until you are done.”
The point is to make sure the rail is put back up before you leave the room
Staff Management
How do you intervene with inappropriate behavior from staff?
This is not prioritizing, this is not delegating … this is handling staff members who did stupid things
There are always 4 answers
- Tell Supervisor
- Confront them and take over the task the staff is implementing immediately
- Talk to them later
- Ignore it
Never ignore inappropriate behaviors … So, “ignore it” is the wrong answer
-
- Use the incident as an opportunity to teach and change behavior
Choosing among the remaining 3 options depends on the nature of the incident … Therefore, ask yourself one of the following?
-
- Is the staff doing something Illegal?
- If answer is YES … Then, Tell Supervisor
- If what the staff is doing is not illegal?
- Then ask yourself if anyone (patient, the co-worker, or other staff member) is in immediate of physical or psychological harm?
- If answer is YES … Confront immediately and take over
- If no one is in harm’s way, ask yourself if this behavior is simply inappropriate
- If so, talk to that particular staff at a later time about the incident
- Is the staff doing something Illegal?
Examples
- You suspect the RN is diverting narcotics. Tell Supervisor
- The Aide is giving perineal care to pt, not wearing gloves? Confront and take over the task
- The RN is going home with bulging pockets? Tell Supervisor
- You notice surgeon contaminates her gloves? Confront
- The RN always gives report, always says exasperation instead of exacerbation …
Talk to them later
If an illegal act can be harmful to the pt … first, takeover the task and then report the incident to supervisor
Questions
What if you find 2 pts involving in sexual intercourse? What is best thing to do?
-
- Shut the door and give then privacy
- As a staff, you do the same if you stumble upon a pt masturbating in his or her room
Organ Location
If a question is asking you to identify a named organ on a picture on the screen, it is a simple point-and-click on the organ on the screen … To do so, move the mouse over the area and click
-
- An “X” identifies the organ you want to select as your answer
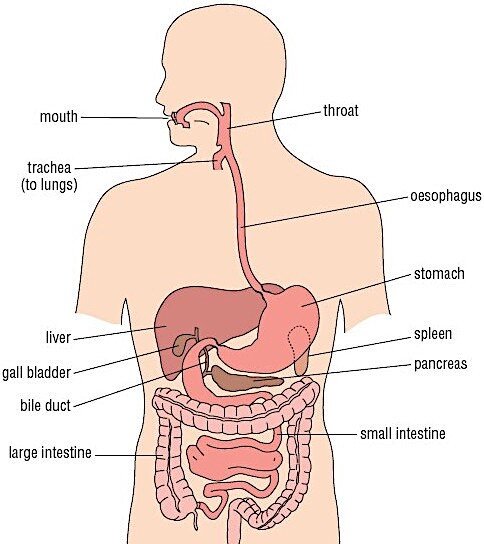 As long as you are in the general vicinity, you will identify the organ, given you are correct
As long as you are in the general vicinity, you will identify the organ, given you are correct
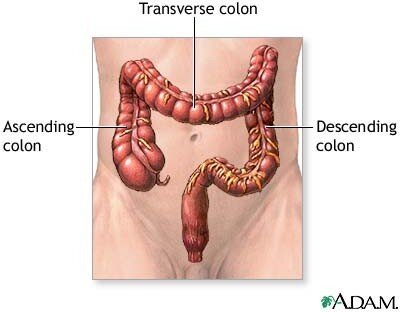
Note
- Not present on both pictures are the brain, lungs and kidneys
- Questions regarding the brain will be more on identifying the lobes with relation to their functions
Auscultation Over Heart Valves
When answering questions to identify heart valves, you must click exactly over a narrow area as to mimic stethoscope placement. The areas auscultated for murmurs (or sounds) are remembered by “A PET M”
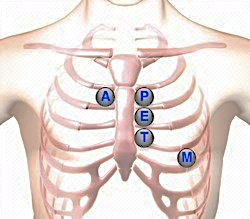
-
- The Aortic valve is located in the 2nd intercostal space, right of the sternal border
- The Pulmonic valve is located in the 2nd intercostal space, left of the sternal border
- The Erb point is rarely asked on the exam
- It is located in the 3rd intercostal space, left of the sternal border
- Erb point is between the pulmonic and the tricuspid valve
- The Tricuspid valve is located in the 4th intercostal space, left of the sternal border
- The Mitral valve is located in the 5th intercostal space at the midclavicular line
- The apical pulse is in the same location as the mitral valve auscultation
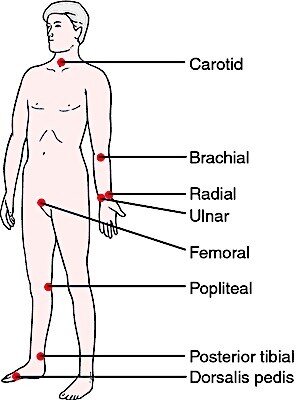 Palpating for Pulses
Palpating for Pulses
Know where on the body these pulses are located
-
- For instance, anticipate questions about identifying the popliteal pulse on a picture on the human body
Guessing Strategies
Everybody taking this exam will guess at some point. Instead of guessing blindly, here are some strategies that can help you answer questions correctly
Use these approaches when all the answers do not make sense …
- In psych nursing
- Pick, “I will examine my feelings”
- This is to prevent countertransference
- Countertransference: A pt reminds a nurse of her dad, who she a bad relation with, so she interacts in a hostile manner with the pt
- Or pick, “Establish a trust relationship”
- Pick, “I will examine my feelings”
- Nutrition
- When all else fails, go with “baked”—not fried—but “backed chicken”
- If there is no chicken, pick fish—not shellfish (lobsters, crabs, or shrimp). Shellfish is high in cholesterol
- Never pick casseroles for children—they won’t eat it
- A casserole is any kind of stew or side dish that is cooked slowly in an oven
- Don’t mix meds in kids food
- Always ask pts for permission before you mix their food and medication together
- For toddlers, pick “finger food”
- Examples are: Hot dogs, tofu, French fries
- Your answer should focus on what can they eat on the run
- For preschoolers, “leave them alone”
- One meal a day is ok
- Growth curve around preschool year plateaus … Toddlers growth curve goes up
- When all else fails, go with “baked”—not fried—but “backed chicken”
- Pharmacology
- Memorize S/E
- Don’t memorize dosage, route
- If you know what a drug does but don’t know the S/E, how do you proceed? … Pick the “S/E in the same body system the drug is working”
- For instance, if you have a GI drug, and drowsiness, tachycardia, and diarrhea are part of the answer choices. What S/E will you pick? Pick “diarrhea”
- From the same above list … For cardiac drug, pick “tachycardia”
- For CNS drug, pick “drowsiness”
- If you have no idea what the drug is … and the drug is PO, pick a GI side-effect
- Never tell a child a “medication is candy”
- The child may give grandma’s valium to other children thinking the pill is candy
- OB: check “fetal heart rate”
- Med/Surge
- What is the first thing to assess? “Check for LOC (level of consciousness)”—not airway
- Think about a code or you find a pt on the floor … LOC is always checked first
- “Sir, Sir, Sir! Are you ok? Can you hear me?” If there is no response, A-B-C is then done next
- What is the first thing to do? “Establish an airway”
- What is the first thing to assess? “Check for LOC (level of consciousness)”—not airway
- Pediatrics
- For growth and development, you can always narrow down your answer to three rules, which goes along “giving the child more time”
- Rule #1: When in doubt, “call it normal” … Example: Some six year olds can read. Some can and some can’t. Pick the answer that says, “Give the child more time” … There is no doubt that a 13-year-old who not potty-trained is normal
- Rule #2: When in doubt, pick the “older age” in the 2 that it could be … In what age can the child walk? Both 12 months and 14 months are right … Pick 14 months. In that case, you give the child more time
- Rule #3: When in doubt, pick the “easier task” … At 6 months, a baby can roll over or sit with support … Pick “roll over” as your answer because it is the easier task.
- In growth and development, there are always two correct answers. The mantra is to give the child more time … Chant in your head: “NORMAL, OLDER, EASIER”
- For growth and development, you can always narrow down your answer to three rules, which goes along “giving the child more time”
- General guessing skills
- “Rule out absolutes” … That is if you are guessing. However, it is commonly known to never push potassium
- Avoid answer choices that say the same thing … Neither one is correct. For instance, the following 2 answer choices are the same. Answer choice #1: Increased bowel sounds … Answer choice #2: borborygmi. Pick a different one
- If two answers are opposite, one is probably correct
- Umbrella strategy … Find more than one correct answer? Find the global answer. Ex: Use safety and good body mechanics if possible
- Prioritization of pt needs
- Pt is need with the worst outcome has the highest priority—in other words, pick the Worst Consequences Game
- For example: Which is highest priority for suicidal patient? (a) Don’t give tranquilizer. (b)
- Pt is need with the worst outcome has the highest priority—in other words, pick the Worst Consequences Game
Don’t orient to unit? (c) Don’t put him on suicide precautions? And (d) Don’t introduce him to staff?
To answer this question, ask yourself is: “What would happen if I did not implement the task?” Answers: (a) Agitated, (b) Lost, (c) DEAD, (d) Doesn’t know anyone. The worse case scenario is (c). The pt would be DEAD. Answer choice (c) is the answer.
- When you’re stuck between two answers … Go back and read question. You probably missed something
- The Sesame Street Rule

- When nothing else works, look at all the answer choices to see which one looks different from the others
- Looking at the picture below, one is not like the others … If that happens on the exam, the answer choice that looks different is likely the right answer
- The wrong answers look the same
- Don’t be tempted to answer based on ignorance rather than knowledge
- If you don’t know drug, pull it out of the question and try to answer based on fundamental knowledge or common sense
o For example: The Piggyback question about Amikacin … You don’t know the medication Amikacin, but you do know that piggybacks need a pump. Don’t analyze those first 10 questions on the NCLEX. USE COMMON SENSE
- The are 3 expectations you are not allowed to have
- Expectation #1: Remember—the test will not be what you expect
- Don’t expect 75 (RN) or 85 (LPN) questions … Go to the exam center and expect 265 or 285 questions
- Prepare yourself to go for the maximum
- If you freak OUT when you get to 76 (RN) or 86 (LPN) and on, it might impact your performance on the exam … Negativity will kill you
- This is a computer-adapted test—if you get to 200 you’re not failing … You’re still in the game!
- Expectation #2: Don’t expect to know everything. It ain’t happening
- Expectation #3: Don’t expect a perfect day
- Perfect parking spot
- Perfect Seat Partner
- You stuck it out through nursing school this far … You have perseverance and strength of character
- Get through one question at a time